
Abstract
Objective: Advances in transcatheter closure device materials ensure safety and long-term effectiveness in most atrial septal defect (ASD) cases.
Methods: This single-center study retrospectively evaluated outcomes in 26 pediatric patients who underwent transcatheter ASD closure between 2023 and 2025. Transcatheter closure was attempted using the Occlutech® Figulla Flex II ASD Occluder (OFSO). Follow-up evaluations of device-specific outcomes, procedural success rates, and complications were recorded.
Results: The average age of the patients was 9.3 ± 4.1 years, and 61.5% were girls. Of the total patients, 11.5% had a large defect. A complication occurred in 1 patient (3.8%).
Conclusion: Transcatheter closure of ASD with the OFSO device is a safe and effective treatment strategy for children, demonstrating a high procedural success rate and an overall complication rate of 3.8%.
Keywords: atrial septal defect, child, transcatheter closure, device
INTRODUCTION
Atrial septal defect (ASD) is one of the most common congenital heart defects, comprising approximately 6–10% of all cases. The secundum type is particularly prevalent and is usually the most suitable for transcatheter closure. The clinical course of secundum ASDs varies; small defects may remain asymptomatic throughout life, while moderate-to-large defects can result in right ventricular volume overload, arrhythmias, and pulmonary overcirculation if left untreated. Closure is generally indicated when the ratio of pulmonary to systemic blood flow (Qp/Qs) exceeds 1.5.1-5
Over the past two decades, percutaneous ASD closure has become the preferred treatment for selected pediatric patients, largely due to its minimally invasive nature and shorter recovery times. The Amplatzer Septal Occluder (ASO) is the most widely used device for this procedure.3 The other devices used for ASD closure are the Cera-Flex Occluder, Occlutech ASD Occluder, Amplatzer Cribriform Occluder, Gore Cardioform Septal Occluder, and Gore Cardioform ASD Occluder.6-14 The results of the Occlutech Figulla Septal Occluder (OFSO) have not been reported as frequently. Haas et al. found that ASD closure using OFSO is feasible in a large variety of patients (in 1315 patients of all age groups) and is safe with only a minimal risk of severe side effects. However, the safety and efficacy of newer or less commonly utilized devices in the pediatric population are still not well established.15 The OFSO devices have important structural differences, especially an absent left atrial hub, and the latest generations have a tiltable delivery system that seems to be advantageous regarding the feasibility of implantation in complex ASDs, device delivery, as well as device alignment to the atrial septum, and thereby echocardiographic assessment during implantation.16 Roymanee et al. found that there were no significant differences between the major and minor complications when comparing the OFSO and ASO devices.17
This study aimed to present our single-center experience with the Occlutech® Figulla Flex II ASD Occluder device for the transcatheter closure of secundum ASDs in children. We focused on evaluating device-specific outcomes, procedural success rates, and complications.
MATERIAL and METHODS
This retrospective study included pediatric patients aged 2 to 18 years who underwent transcatheter closure of secundum ASDs with the Occlutech® Figulla Flex II ASD Occluder device at the İzmir City Hospital from 2023 to 2025. Several ASD devices, such as Amplatzer, CERA, and OFSO, are used in our center. The OFSO is preferred over other devices due to its ease of use for both the operator and previous ASD closure options. Because the OFSO connector allows for free rotation up to 50 degrees and angulation without requiring any force, the device is easier to insert. Therefore, it is frequently preferred by operators. This study was conducted solely to share our experiences with the OFSO. All procedures presented in this study were performed by the same two interventional cardiologists.
Inclusion criteria were secundum ASD greater than 8 mm, Qp/Qs ratio greater than 1.5, and enlargement of the right heart structures. Exclusion criteria were an echocardiographic (ECO) diameter greater than 30 mm and inadequate inferior and posterior rims.
The cohort consisted of 16 girls and 10 boys, all of whom exhibited significant left-to-right shunting as confirmed by echocardiography and demonstrated evidence of right heart volume overload. Importantly, none of the patients presented with severe pulmonary hypertension. The institutional ethics committee approved the study (Approval Number: 2025/392).
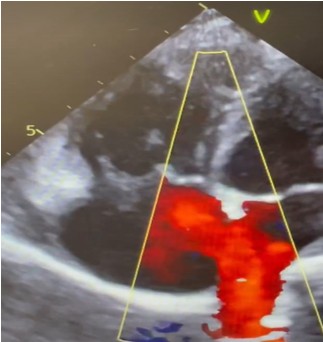
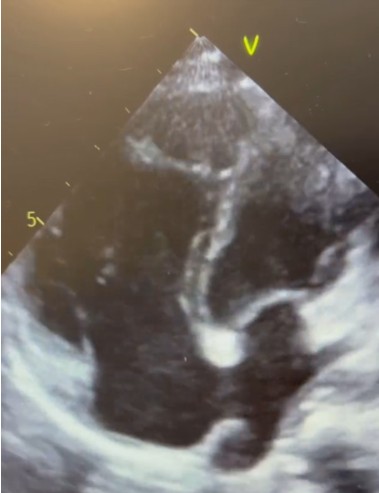
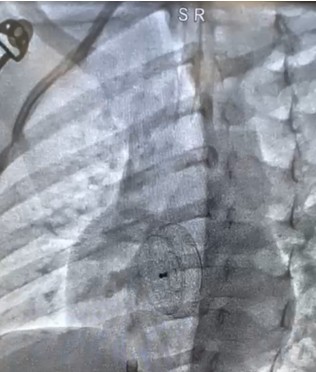
Demographic data, body surface area (BSA), ECO diameter, mean-PAP, right ventricular end-diastolic (RVED) diameter, device size, fluoroscopy time, Qp-Qs, defect diameter (with transesophageal echocardiography), balloon sizing, total septum diameter, rim adequacy, defect size/total septum diameter, defect size/weight, defect size/BSA were recorded. Pre-procedure echocardiographic evaluations were performed using either transthoracic (TTE) (Figure 1 and Figure 2) or transesophageal echocardiography (TEE), based on the patient’s weight. Balloon sizing was conducted in all cases (Figure 3).

Procedure
The procedure was performed under general anesthesia in a pediatric catheterization lab. Occlutech® Figulla ASD Occluder was used in all cases (Figure 4). A large defect is defined as one with a diameter-to-weight ratio greater than 1.2 or a diameter-to-BSA ratio exceeding 20 mm/m². Post-procedural care included 24 hours of in-hospital observation, acetylsalicylic acid for six months, and prophylaxis for infective endocarditis for one year. Follow-up evaluations, including ECG, echocardiography (Figure 5), were scheduled at one week, one month, three months, and six months. The procedural complications, such as device embolization and arrhythmia, were evaluated. The presence of a residual shunt was assessed by color Doppler using TTE.

Statistical analysis
Statistical analysis was conducted using SPSS version 23.0. Categorical variables were reported as frequencies and percentages, while continuous variables were presented as means with standard deviations.
RESULTS
Demographics
A total of 26 patients were included in the study. The mean age was 9.3 ± 4.1 years, 61.5% were female, and 11.5% had congenital heart disease. The average body weight was 34.8 ± 19.1 kg (Table 1). Before the procedure, 73.1% of the patients had right bundle branch block, 3.8% had complete AV block, and 23.1% had normal ECGs.
| *Aortic Coarctation, Ventricular Septal Defect, Congenital AV block. | ||||
| Table 1. Patient characteristics | ||||
|
|
|
|
|
|
| Age (year) |
|
|
||
| Weight (kg) |
|
|
||
| Height (cm) |
|
|
||
| Gender | ||||
| Female |
|
|
||
| Male |
|
|
||
| Congenital Heart Disease | ||||
| No |
|
|
||
| Yes* |
|
|
||
Procedure results
The ASD diameter was assessed using TTE before the procedure, as shown in Figure 1 and Figure 2. Figure 1 shows an echocardiographic image of a patient with a 16-mm ASD. Figure 2 shows an image of a patient with enlargement of the right heart structures using TTE. ASD diameter was measured with balloon sizing in all patients. Figure 3 shows an image of a patient who underwent balloon sizing.
The mean echocardiographic ASD diameter was 12.7 ± 2.9 mm, while the mean balloon-stretched diameter measured 15.0 ± 4.8 mm. The average device size used was 16.0 ± 5.2 mm. In terms of procedural metrics, the mean fluoroscopy time was 9.0 ± 2.1 minutes. Regarding hemodynamic measurements, the average Qp/Qs ratio was 1.7 ± 0.1 (Table 2).
| *ECO: Echocardiography, PAP: Pulmonary artery pressure, BSA: Body surface area, RVED: Right ventricular end-diastolic. | ||
| Table 2. Procedure characteristics | ||
|
|
|
|
| ECO diameter (mm) |
|
|
| Mean-PAP (mm-hg) |
|
|
| Right ventricular end-diastolic (RVED) diameter (mm) |
|
|
| Device size (mm) |
|
|
| Fluoroscopy time (min) |
|
|
| Qp-Qs |
|
|
| Defect diameter (TEE) (mm) |
|
|
| Balloon-stretched diameter (mm) |
|
|
| Total septum diameter (mm) |
|
|
| Defect size/total septum diameter |
|
|
| Defect size/weight |
|
|
| Defect size/body surface area |
|
|
Out of the total patients, 3 (11.5%) were identified as having a large defect. Deficient rims were observed in 7 patients (26.9%), with the aortic rim being the most affected in 6 patients, and the inferoposterior rim was affected in 1 patient. OFSO was placed in 25 patients without complications. Figure 4 shows a fluoroscopy image after release of the OFSO device in a patient with an 18 mm ASD. Figure 5 shows an image of a patient in whom OFSO was placed without creating aortic compression.
The patient with complications (n = 1) had a small defect, while three of the patients without complications (n = 25) had large defects, and the other 22 patients had small defects. The patient with complications had an insufficient rim, while six of the patients without complications (24%) had insufficient rims. There was no residual shunt in the patient with complications, whereas one of the patients without complications (4%) had a residual shunt.
When comparing patients with and without complications, the patient with complications (n = 1) had a small defect, while three of the patients without complications (n = 25) had large defects, and the other 22 patients had small defects. The patient with complications had an insufficient rim, while six of the patients without complications (24%) had insufficient rims. There was no residual rim in the patient with complications, whereas one of the patients without complications (4%) had a residual rim.
Complications occurred in only one patient (3.8%), resulting in device embolization. On the first day after the procedure, an echocardiogram revealed that the device had embolized into the ascending aorta. The patient underwent further angiography, and attempts were made to retrieve the device with a snare. Because the device could not be removed, the patient was referred for surgery. The device was removed from the aorta, and the ASD was surgically closed. In another patient, the device was not placed due to the insufficient and flexible inferior vena cava (IVC) rim, and the patient was referred for surgery. During the follow-up, no residual shunt was observed in any of the patients.
DISCUSSION
This single-center, retrospective study presented our OFSO device experience in the transcatheter closure of secundum ASD in a pediatric population. Our findings confirmed that percutaneous closure of ASD with the OFSO device is a safe and effective treatment strategy for children, demonstrating a high procedural success rate and a complication rate of 3.8%. A key strength of this study was the evaluation of OFSO devices in real-world pediatric use. These results aligned with prior large-scale studies, including multicenter registries and device-specific trials, which report complication rates ranging from 3% to 7% in pediatric and mixed-age populations. However, there are limitations due to the small sample size (n = 26) and single-center design.
Roymanee et al. found that OFSO devices were safe and effective for percutaneous ASD closure (success rate: 97.4%). The OFSO had the benefit of a shorter fluoroscopic time (ASO 13.7 min; OFSO 9.0 min).17 In our study, the mean fluoroscopy time was 9.0 ± 2.1 minutes.
In our study, device embolization occurred in one patient who had a deficient rim and large defects. As previously noted by Santoro et al. and Sommer et al., deficiencies in the retro-aortic or posterior rims significantly elevate the risk of device instability and migration.9,10 In our study, the device was not placed due to the insufficient and flexible IVC rim in one patient, and the patient was referred for surgery. In other patients, no residual shunt was observed during the follow-up. In another mixed-group study comparing the devices, 6 (3%) patients in the OFSO group had a large residual shunt, and 12 (6%) had a small residual shunt. In the ASO group, 5 (3%) patients had a large residual shunt, and 19 (10%) had a small residual shunt. The prevalence of a residual shunt did not differ between the two groups.18
Although rare, AV block is one of the most feared complications of ASD closure, particularly in small children and those with oversized devices relative to their body size. In our cohort, we did not observe AV block. Houeijeh et al. and Muroke et al. noted that AV block occurred in up to 1% of patients, especially those with oversized devices.11,12 Our results highlighted the importance of carefully considering the device-to-weight and device-to-septal diameter ratios during patient selection, particularly for children weighing under 15 kg or those with large defects.
The study found that a large ASD, defined as a defect size-to-body surface area ratio greater than 20 mm/m² or a defect size-to-weight ratio greater than 1.2, was present in 11.5% of patients. While most of these patients achieved successful closure, our findings aligned with prior literature12-14, indicating that large ASDs should be approached with increased caution and meticulous planning. In another study, successful implantation with OFSO was achieved in all pediatric patients, and neither residual shunt nor conduction abnormality was observed in any case.19 This study emphasized the importance of long-term follow-up. Residual shunts were not identified in patients. Notably, during the 6-month follow-up, no cases of device erosion or late-onset pericardial effusion were observed. This may suggest that modern imaging and sizing protocols are effective in preventing these rare but serious complications.
Limitations
Despite its strengths, this study had several limitations. The retrospective, single-center design may restrict its generalizability. This study presented results for up to 6 months. Another limitation of this study was the short follow-up period; these patients need to be observed for a longer term to establish the safety of the device with long-term use. Additionally, the small number of patients limited our ability to draw definitive conclusions about their safety profiles. Nonetheless, these findings offer valuable real-world insights into the OFSO device, procedural planning, and complications in pediatric ASD closure.
CONCLUSION
In conclusion, our experience indicated that transcatheter ASD closure with the OFSO device is a reliable and safe procedure for children. Although major complications such as device embolization were rare (3.8%), they require prompt recognition and management. Future multicenter, randomized, prospective studies are essential to further define the optimal device choice and procedural strategies for anatomically complex defects and for younger pediatric patients.
Ethical approval
This study was approved by the Medical Research Ethics Committee of İzmir City Hospital (Decision/Protocol No: 2025/392). Informed consent was obtained from all participants involved in this study.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declare that this study received no funding.
Generative AI statement
The authors declare that no generative AI or AI-assisted technologies were used in the writing or preparation of this study.
References
- Villablanca PA, Briston DA, Rodés-Cabau J, et al. Treatment options for the closure of secundum atrial septal defects: a systematic review and meta-analysis. Int J Cardiol. 2017;241:149-55. https://doi.org/10.1016/j.ijcard.2017.03.073
- Faccini A, Butera G. Atrial septal defect (ASD) device trans-catheter closure: limitations. J Thorac Dis. 2018;10:S2923-30. https://doi.org/10.21037/jtd.2018.07.128
- Kashyap T, Sanusi M, Momin ES, et al. Transcatheter occluder devices for the closure of atrial septal defect in children: how safe and effective are they? A systematic review. Cureus 2022;14:e25402. https://doi.org/10.7759/cureus.25402
- Everett AD, Jennings J, Sibinga E, et al. Community use of the amplatzer atrial septal defect occluder: results of the multicenter MAGIC atrial septal defect study. Pediatr Cardiol. 2009;30:240-7. https://doi.org/10.1007/s00246-008-9325-x
- Feltes TF, Bacha E, Beekman RH, et al. Indications for cardiac catheterization and intervention in pediatric cardiac disease: a scientific statement from the American Heart Association. Circulation. 2011;123:2607-52. https://doi.org/10.1161/CIR.0b013e31821b1f10
- Wood KP, Fleming GA, Chamberlain RC. Update on transcatheter device closure of congenital septal defects. Curr Cardiol Rep. 2023;25:1083-93. https://doi.org/10.1007/s11886-023-01925-3
- Turner DR, Owada CY, Sang CJ, Khan M, Lim DS. Closure of secundum atrial septal defects with the AMPLATZER Septal Occluder: a prospective, multicenter, post-approval study. Circ Cardiovasc Interv. 2017;10:e004212. https://doi.org/10.1161/CIRCINTERVENTIONS.116.004212
- El-Said H, Hegde S, Foerster S, et al. Device therapy for atrial septal defects in a multicenter cohort: acute outcomes and adverse events. Catheter Cardiovasc Interv. 2015;85:227-33. https://doi.org/10.1002/ccd.25684
- Santoro G, Pizzuto A, Cuman M, et al. Transcatheter closure of “surgical” ostium secundum atrial septal defects with Gore Cardioform ASD Occluder. J Card Surg. 2022;37:3200-6. https://doi.org/10.1111/jocs.16786
- Sommer RJ, Love BA, Paolillo JA, et al. ASSURED Clinical Study: new Gore Cardioform Asd Occluder for transcatheter closure of atrial septal defect. Catheter Cardiovasc Interv. 2020;95:1285-95. https://doi.org/10.1002/ccd.28728
- Houeijeh A, Hascoët S, Bouvaist H, et al. Transcatheter closure of large atrial septal defects (ASDs) in symptomatic children with device/weight ratio ≥1.5. Int J Cardiol. 2018;267:84-7. https://doi.org/10.1016/j.ijcard.2018.05.069
- Muroke V, Jalanko M, Haukka J, et al. Outcome of transcatheter atrial septal defect closure in a nationwide cohort. Ann Med. 2023;55:615-23. https://doi.org/10.1080/07853890.2023.2178669
- Naseem JA, Riyaz MSU, Joseph SP, et al. Transcatheter closure of large ostium secundum atrial septal defects in symptomatic small children: a single-center retrospective study. Ann Pediatr Cardiol. 2023;16:393-8. https://doi.org/10.4103/apc.apc_163_23
- El-Sisi AM, El-Saiedi SA, Ammar R, Abdelhameed A, Hijazi ZM, Soliman MM. Safety of Occlutech Septal Occluder ACCELL Flex II for transcatheter closure of secundum atrial septal defects in children: a long-term follow-Up. J Interv Cardiol. 2022;2022:8886813. https://doi.org/10.1155/2022/8886813
- Haas NA, Soetemann DB, Ates I, et al. Closure of secundum atrial septal defects by using the Occlutech occluder devices in more than 1300 patients: The IRFACODE project: a retrospective case series. Catheter Cardiovasc Interv. 2016;88:571-81. https://doi.org/10.1002/ccd.26497
- Haas NA, Happel CM, Soetemann DB, et al. Optimal septum alignment of the Figulla Flex occluder to the atrial septum in patients with secundum atrial septal defects. EuroIntervention. 2016;11:1153-60. https://doi.org/10.4244/EIJY14M12_09
- Roymanee S, Promphan W, Tonklang N, Wongwaitaweewong K. Comparison of the Occlutech Figulla septal occluder and Amplatzer septal occluder for atrial septal defect device closure. Pediatr Cardiol. 2015;36:935-41. https://doi.org/10.1007/s00246-015-1103-y
- Nakayama R, Takaya Y, Akagi T, et al. Efficacy and safety of atrial septal defect closure using Occlutech Figulla Flex II compared with Amplatzer Septal Occluder. Heart Vessels. 2021;36:704-9. https://doi.org/10.1007/s00380-020-01739-1
- Mortezaeian H, Sayadpour Zanjani K, Malakan Rad E. Transcatheter atrial septal defect closure using occlutech figulla device: a two-center experience. J Tehran Heart Cent. 2013;8:197-201.
Copyright and license
Copyright © 2026 The author(s). This is an open-access article published by Aydın Pediatric Society under the terms of the Creative Commons Attribution License (CC BY) which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.
