
Abstract
Acute urinary retention is an uncommon clinical condition in childhood and adolescence and is typically linked to neurological, infectious, or structural causes. Hematometrocolpos secondary to imperforate hymen is a well-recognized gynecologic condition that may be overlooked and may present with urinary retention, particularly in adolescents.
We report the case of a 12-year-old girl with no significant past medical history who presented to the pediatric emergency department with suprapubic pain and an inability to void. Despite clear pubertal development (Tanner stage IV), she had primary amenorrhea. Pelvic imaging demonstrated a large fluid-filled mass consistent with hematometrocolpos due to an imperforate hymen. Hymenotomy was performed with drainage of approximately 500 mL of retained menstrual blood. The postoperative course was uneventful, and spontaneous menstruation began three weeks later.
This case highlights the educational value of recognizing gynecologic causes of urinary retention, particularly in emergency settings where the diagnosis may be missed due to the predominance of urologic and neurologic considerations. A careful physical examination in pubertal girls presenting with acute urinary retention, especially in the presence of primary amenorrhea and cyclic abdominal pain, is essential to ensure early diagnosis and to avoid unnecessary investigations and delays in management.
Keywords: urinary retention, hematometrocolpos, imperforate hymen, primary amenorrhea, adolescent
INTRODUCTION
Acute urinary retention is an uncommon clinical condition in adolescents and is most commonly associated with neurological disorders, urinary tract infections, urolithiasis, or structural anomalies.1-3 Gynecologic causes, although less frequent, should be considered in selected patients, particularly in those with pubertal development and primary amenorrhea accompanied by cyclic pelvic pain and voiding difficulty.2,3 Imperforate hymen, the most common congenital obstructive anomaly of the female genital tract, has an estimated incidence of 0.014%–0.1% (approximately 1 in 1,000 to 1 in 10,000 females), and represents a well-recognized clinical entity that may nevertheless be overlooked in acute care settings.1,2
Hematometrocolpos is a congenital obstructive anomaly usually caused by an imperforate hymen and typically presents with primary amenorrhea, abdominal pain, pelvic distension, and occasionally low back pain.1-4 Although cyclic pelvic pain and abdominal mass are common features, acute urinary retention as the initial manifestation is an infrequent but clinically important presentation.5-7 Providing this epidemiologic context is essential for understanding why atypical presentations, such as urinary retention, warrant careful diagnostic consideration.
Ultrasonography is the first-line imaging modality because it reliably identifies pelvic fluid collections and reproductive tract distension.7 Magnetic resonance imaging (MRI), however, provides superior delineation of the level and extent of obstruction, as well as its relationship with adjacent pelvic structures.8 Delayed diagnosis may result in serious sequelae, including endometriosis, hydronephrosis, and even infertility.8,9
Here, we describe an adolescent girl with hematometrocolpos who presented with acute urinary retention, highlighting the educational value of this presentation and the importance of considering gynecologic causes in the differential diagnosis, particularly in emergency settings where early recognition can prevent unnecessary investigations and delays in management.
CASE PRESENTATION
A 12-year-old previously healthy girl presented to the pediatric emergency department with suprapubic pain and inability to void urine. She had no history of medication use or systemic illness. Despite pubertal development consistent with Tanner stage IV, she had primary amenorrhea. She reported intermittent lower abdominal pain over the past three months, which had progressively worsened over the preceding two days, culminating in acute urinary retention. One month earlier, she had been evaluated at another hospital for similar symptoms but was discharged without a definitive diagnosis.
On examination, the patient was hemodynamically stable. Physical assessment was unremarkable except for a palpable suprapubic mass consistent with bladder distension. Laboratory tests, including complete blood count, biochemical profile, and urinalysis, were within normal limits, and serum β-hCG was negative.
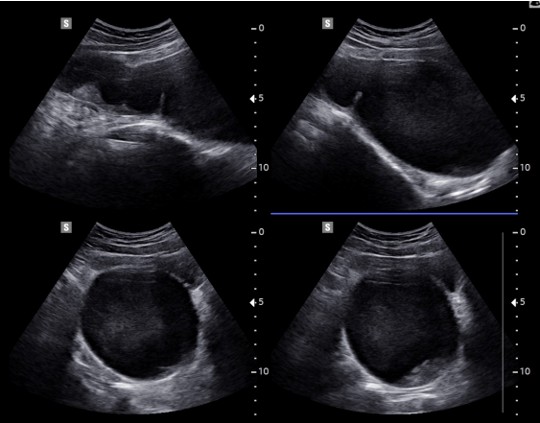
A Foley catheter was inserted, draining approximately 700 mL of urine, which relieved her symptoms. Pelvic ultrasonography revealed a large, homogeneous, echogenic collection measuring 17 × 7.5 cm, extending from the endometrial cavity and cervix into the vaginal canal to the hymenal level, consistent with hematometrocolpos (Figure 1). The Foley catheter was left in place for approximately 12 hours preoperatively to ensure decompression and symptomatic relief. A single preoperative prophylactic dose of intravenous cefazolin was administered, and analgesia was achieved with weight-based intravenous paracetamol, which adequately controlled her pain.
A detailed external genital examination performed by a gynecologist revealed a tense, bulging, bluish imperforate hymen, and the diagnosis was subsequently confirmed during gynecologic evaluation. Pelvic contrast-enhanced MRI demonstrated a markedly distended uterus reaching the level of the umbilicus (22 × 9 cm), with a thinned myometrium and markedly distended endometrial and vaginal cavities filled with hematic content. The bladder was displaced anteriorly with reduced capacity (Figure 2).

The patient underwent hymenotomy under general anesthesia via cruciate incision, resulting in drainage of approximately 500 mL of retained menstrual blood. Hemostasis was secured, mucosal eversion was achieved, and a vaginal Foley catheter was placed to prevent restenosis. The postoperative course was uneventful. She was discharged on postoperative day 3, and at follow-up, she reported complete resolution of symptoms. Menstruation commenced spontaneously three weeks after the procedure.
DISCUSSION
Acute urinary retention in adolescence is an uncommon clinical presentation and is typically related to neurological, infectious, lithiasis-related, or structural causes.1-3 Gynecologic etiologies, though less frequently considered, should be included in adolescent girls with pubertal development, primary amenorrhea, cyclic pelvic pain, and voiding difficulties. In this context, the differential diagnosis should be approached systematically and should include neurologic disorders such as spinal cord lesions, tethered cord syndrome, transverse myelitis, or Guillain–Barré syndrome; infectious etiologies including severe cystitis, vulvovaginitis, or pelvic inflammatory disease; and mechanical or obstructive causes such as urolithiasis or urethral anomalies. Psychological or functional conditions—such as dysfunctional voiding, psychogenic urinary retention, or acute anxiety—may also mimic obstructive symptoms.1-3 In addition, medication-related urinary retention, particularly associated with anticholinergic drugs, antihistamines, or psychotropic agents, should be considered when relevant. Recognizing this broad range of potential causes is essential to avoid misdiagnosis and ensure timely identification of structural gynecologic conditions that may otherwise be overlooked, especially when clinical features such as primary amenorrhea and cyclic pelvic pain are present.
Hematometrocolpos, most often secondary to imperforate hymen, is a well-recognized congenital anomaly. The classical presentation includes primary amenorrhea and abdominal or pelvic pain; however, urinary retention as the predominant symptom represents an infrequent but clinically important manifestation.4-7 This case emphasizes the educational value of recognizing this presentation, particularly for clinicians working in emergency and primary care settings, where urologic and neurologic causes are often considered first.
Previous reports have highlighted similar presentations: Ercan et al.5 and Asikhia et al.6 described adolescents with hematometrocolpos complicated by acute urinary retention, while Santos et al.7 emphasized the role of imaging in diagnosis. Niang et al.8 demonstrated that delayed recognition may lead to hydronephrosis and endometriosis, and Liang et al.9 confirmed favorable long-term outcomes following surgical correction. More recently, Al-Bulushi et al.10 described a comparable case successfully managed with hymenotomy. Collectively, these reports indicate that early recognition is the key determinant of positive clinical outcomes.
In emergency department settings, acute urinary retention in adolescent girls is often evaluated from a urologic or neurologic perspective, which may delay recognition of underlying gynecologic causes. Early identification of conditions such as hematometrocolpos can markedly change clinical management by preventing unnecessary investigations and expediting definitive treatment. A careful physical examination—particularly in pubertal girls presenting with urinary retention accompanied by primary amenorrhea or cyclic pelvic pain—is therefore essential to avoid diagnostic delay and optimize patient outcomes.5-9
Ultrasound remains the first-line diagnostic modality due to its accessibility and sensitivity in identifying pelvic masses. MRI, however, is indispensable in delineating the extent of obstruction and its impact on adjacent pelvic structures, as in our case, where anterior displacement of the bladder explained the retention.7,8 In emergency department settings, a diagnostic approach that begins with a careful physical examination and is supported by timely imaging is essential to prevent unnecessary investigations and delays in appropriate management.
Failure to diagnose promptly may result in retrograde menstruation, endometriosis, urinary tract obstruction, and infertility.8,9 Notably, our patient had previously been evaluated elsewhere without a correct diagnosis, illustrating the potential for misdiagnosis. Early recognition is particularly crucial in both primary care and emergency departments, as an imperforate hymen is a fully correctable cause of acute urinary retention when identified promptly. Delayed diagnosis, however, may lead not only to avoidable investigations and repeated healthcare visits but also to preventable complications such as hematosalpinx, endometriosis, hydronephrosis, and infertility.8,9 These observations highlight the importance of sustaining heightened clinical vigilance and conducting a comprehensive physical examination in pubertal female patients who present with urinary retention.
Surgical hymenotomy is the gold-standard treatment, with cruciate or annular incisions most commonly employed.4-6,10 In this case, cruciate hymenotomy successfully relieved symptoms, with no recurrence or postoperative complications.
Hematometrocolpos should therefore be considered in the differential diagnosis of acute urinary retention in adolescent girls presenting with primary amenorrhea and pubertal development. This report emphasizes the educational value of this clinical presentation and highlights the importance of maintaining a high level of clinical awareness for early recognition. Clinicians evaluating adolescents with urinary retention should remain attentive to gynecologic etiologies, particularly when symptoms are accompanied by cyclic pain or menstrual abnormalities, to facilitate timely intervention and prevent potentially serious long-term complications.
Ethical approval
Written informed consent was obtained from the patient(s) or their legal guardians for the publication of this study and any accompanying images.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declare that this study received no funding.
Generative AI statement
The authors declare that during the preparation of this study, the following AI-assisted technology was used: ChatGPT (OpenAI) in October 2025. Extent of Use: To assist with language editing and improving the clarity of expression. The authors confirm that they have critically reviewed and edited any AI-generated content and take full responsibility for the integrity, accuracy, and originality of the publication. The authors certify that the original human contribution is maintained and that AI-assisted tools are not listed or cited as authors.
References
- Parazzini F, Cecchetti G. The frequency of imperforate hymen in northern Italy. Int J Epidemiol. 1990;19:763-4. https://doi.org/10.1093/ije/19.3.763
- Lee KH, Hong JS, Jung HJ, et al. Imperforate hymen: a comprehensive systematic review. J Clin Med. 2019;8:56. https://doi.org/10.3390/jcm8010056
- Dietrich JE, Millar DM, Quint EH. Obstructive reproductive tract anomalies. J Pediatr Adolesc Gynecol. 2014;27:396-402. https://doi.org/10.1016/j.jpag.2014.09.001
- Kumar Y, Yadav P, Agarwal A. Abdominal swelling and obstructive uropathy due to hematometrocolpos secondary to imperforate hymen: a case report. Pan Afr Med J. 2022;41:18. https://doi.org/10.11604/pamj.2022.41.18.32582
- Ercan CM, Karasahin KE, Alanbay I, Ulubay M, Baser I. Imperforate hymen causing hematocolpos and acute urinary retention in an adolescent girl. Taiwan J Obstet Gynecol. 2011;50:118-20. https://doi.org/10.1016/j.tjog.2011.01.005
- Asikhia O, Durrani M, Dugas C, Cackovic C, Jerusik B. Imperforate hymen and hematometrocolpos in a female with back pain and urinary retention. Cureus. 2022;14:e30525. https://doi.org/10.7759/cureus.30525
- Santos XM, Krishnamurthy R, Bercaw-Pratt JL, Dietrich JE. The utility of ultrasound and magnetic resonance imaging versus surgery for the characterization of müllerian anomalies in the pediatric and adolescent population. J Pediatr Adolesc Gynecol. 2012;25:181-4. https://doi.org/10.1016/j.jpag.2011.12.069
- Niang I, Diouf KN, Thiam M, et al. Late diagnosis of imperforate hymen with hematometrocolpos and bilateral hydronephrosis of a horseshoe kidney. Radiol Case Rep. 2020;15:2217-20. https://doi.org/10.1016/j.radcr.2020.08.054
- Liang CC, Chang SD, Soong YK. Long-term follow-up of women who underwent surgical correction for imperforate hymen. Arch Gynecol Obstet. 2003;269:5-8. https://doi.org/10.1007/s00404-002-0423-3
- Al-Buloushi N, AlBusairi S, Alenezi A, Zahir M. Urinary retention complicated by hematocolpos in an adolescent girl: case report. Int J Surg Case Rep. 2023;112:108934. https://doi.org/10.1016/j.ijscr.2023.108934
Copyright and license
Copyright © 2026 The author(s). This is an open-access article published by Aydın Pediatric Society under the terms of the Creative Commons Attribution License (CC BY) which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.
