
Abstract
Objective: The coexistence of psoriasis and juvenile‑onset systemic lupus erythematosus (jSLE) is rare, and data on familial aggregation of psoriasis across pediatric rheumatic diseases are limited. This study evaluated the co-existence of psoriasis in jSLE, its familial clustering, and its association with the jSLE phenotype.
Methods: In this single‑center cross‑sectional study, patients with jSLE, familial Mediterranean fever (FMF), and juvenile systemic sclerosis (jSSc) were systematically screened for personal and family histories of psoriasis. Recurrence risk ratios for psoriasis were calculated separately for patients and their relatives within each disease group. Among patients with jSLE, clinical manifestations, laboratory parameters, and disease activity (SLEDAI‑2K) were compared between those with and without personal and/or familial psoriasis.
Results: Of 189 patients with pediatric rheumatic diseases included, 94 (49.7%) had jSLE, 73 (38.6%) had FMF, and 22 (11.7%) had jSSc; 69.3% were female, with a higher frequency in jSLE patients (85.1%). Overall, 7,034 individuals (patients and relatives) were systematically screened for psoriasis. Psoriasis was identified in 4 patients (2.1%), all with jSLE (4.3%), and in 25 relatives (0.36%), yielding an overall prevalence of 0.41%. The combined prevalence of psoriasis in jSLE patients and their relatives (0.54%) was significantly higher than in FMF (0.35%) and jSSc (0%) families (p = 0.034). Recurrence risk ratios (λ) for psoriasis in jSLE families were 10.13 for patients and 3.07, 1.16, and 0.67 for first‑, second‑, and third‑degree relatives, respectively; corresponding λ values in FMF families were 0, 1.88, 1.11, and 0.45. Among 94 patients with jSLE, 20 had a personal or family history of psoriasis. However, their clinical signs, laboratory results, and SLEDAI-2K scores showed no significant differences compared with those without a history of psoriasis (p > 0.05).
Conclusion: A positive family history of psoriasis is more common in jSLE than in FMF or jSSc, supporting the hypothesis of a shared genetic background between psoriasis and jSLE, but it was not associated with more severe jSLE in this cohort. These findings underscore the importance of routinely assessing familial psoriasis in jSLE and related disorders and warrant confirmation in larger, prospective, population‑based studies.
Keywords: autoimmunity, FMF, jSLE, jSSc, prevalence, psoriasis, recurrence rate
INTRODUCTION
Autoimmune diseases are chronic, often systemic inflammatory disorders characterized by a persistent and inappropriate immune response by B and T lymphocytes against self-antigens in genetically susceptible individuals, influenced by environmental triggers. Viewed separately, most autoimmune diseases are considered orphan diseases; however, approximately 5% of the general population is affected by one or more autoimmune conditions.1
Two inflammatory diseases with an autoimmune background are psoriasis and systemic lupus erythematosus (SLE). Despite their distinct cutaneous manifestations, both disorders are associated with an increased risk of co-occurrence with other autoimmune diseases compared with the general population.2 Psoriasis affects approximately 3% of people worldwide, usually appearing in the second decade of life and primarily driven by T-lymphocyte-mediated immune dysfunction. However, a prevalence study in Türkiye reported a lower rate of 0.42%.2,3
Systemic lupus erythematosus (SLE) is an autoimmune disease caused by a combination of genetic, environmental, and hormonal factors leading to immunologic abnormalities. SLE affects mainly women during childbearing age, but in approximately 20% of all cases, the diagnosis is first established during childhood and is called juvenile-onset SLE (jSLE).4,5
Familial aggregation of autoimmune diseases suggests shared genetic predisposition and common environmental exposures. Indeed, concurrent cases of SLE and other autoimmune diseases within the same families have been repeatedly reported.6-8 These observations raise the possibility that certain autoimmune conditions may cluster together in families due to overlapping pathogenic mechanisms.
This study is, to our knowledge, the first to evaluate the familial recurrence rates of psoriasis among patients with jSLE, familial Mediterranean fever (FMF), and juvenile systemic sclerosis (jSSc) followed in a pediatric rheumatology outpatient clinic. We selected these diseases because of their distinct pathogenetic pathways, which facilitate the investigation of whether familial aggregation of psoriasis occurs across different pediatric rheumatic and autoimmune disorders.
MATERIALS and METHODS
Study design
This retrospective cross-sectional study included patients attending the pediatric rheumatology outpatient clinic at Istanbul University-Cerrahpasa, Cerrahpasa Faculty of Medicine, between 2023 and 2025, whose clinical and familial data were collected from medical records and subsequently confirmed during follow-up visits.
Patient selection
Patients with jSLE, FMF, and jSSc who were regularly followed at our outpatient clinic were included. FMF patients who met the Eurofever classification criteria and had genetic confirmation were included. Genetic confirmation was defined as the presence of homozygous or compound-heterozygous pathogenic variants in exon 10 of the Mediterranean FeVer (MEFV) gene.9 All patients with jSLE and jSSc met the American College of Rheumatology (ACR)/ European Alliance of Associations for Rheumatology (EULAR) 2019 criteria for SLE10 before 18 years of age and the Pediatric Rheumatology European Society (PReS)/ACR/EULAR provisional criteria for jSSc.11 Patients with overlap syndrome or mixed connective tissue disease, early-onset SLE with monogenic inheritance, and those with irregular follow-up were excluded from the study. Based on these exclusion criteria, the jSLE cohort comprised 94 patients from the initial 142.
Familial psoriasis history was systematically assessed during outpatient visits, supplemented by follow-up contact with relatives when necessary, and confirmed at the patient’s final outpatient visit. The diagnosis of psoriasis in both patients and their affected family members was clinically established and confirmed by dermatologists. Relatives were classified as first-, second-, or third-degree relatives according to standard definitions. First-degree relatives (FDR) included parents, children, and siblings. Second-degree relatives (SDR) encompassed grandparents, grandchildren, aunts, uncles, nephews, nieces, and half-siblings. Third-degree relatives (TDR) included first cousins, great-aunts, great-uncles, grandnephews, grandnieces, great-grandparents, and great-grandchildren.
To avoid family-level clustering, only one individual per family was included in the study. We excluded patients with a known monogenic/genetic diagnosis of SLE and ensured that no first-, second-, or third-degree relatives (including siblings and cousins) of enrolled patients were included in the cohort. Thus, the final sample of 189 jSLE, FMF, and jSSc patients represented unrelated individuals.
jSLE patients with a personal or familial history of psoriasis were compared with those without psoriasis. Clinical, laboratory, immunological characteristics, and disease activity as assessed by the SLE Disease Activity Index 2000 (SLEDAI-2K) were analyzed between the two groups.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics for Mac, Version 31.0 (IBM Corp., Armonk, NY, USA). Categorical variables were summarized as frequencies and percentages (%), whereas continuous variables were presented as mean ± standard deviation (SD) for normally distributed data or as median with interquartile range (IQR, Q1–Q3) for non-normally distributed data. Normality of continuous variables was assessed using histograms and the Kolmogorov-Smirnov test.
For comparisons between two independent groups, the Mann–Whitney U test was used for non-normally distributed continuous variables, whereas the independent-samples t-test was used for normally distributed continuous variables. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. Where prevalence rates across more than two groups were compared and expected cell counts were low, the Fisher–Freeman–Halton exact test with Monte Carlo simulation (10,000 sampled tables) was used instead of Fisher’s exact test.
The recurrence rate (λ) was calculated as the ratio of relatives affected by psoriasis (number of relatives affected by psoriasis divided by the total number of relatives in that category), normalized by the prevalence of psoriasis in the general Turkish population (0.42% according to the Havsa study). The relative recurrence rate of psoriasis was calculated for each degree of relationship among patients with jSLE and FMF, because jSSc had no measurable psoriasis frequency (λ = 0 in both relatives). To assess statistical significance, Fisher’s exact test or the chi-square test was used to compare the proportion of affected relatives in each degree-of-relation group with a hypothetical general population proportion, assuming the same number of relatives. All statistical tests were two-sided, and a p-value < 0.05 was considered statistically significant.
Ethics approval
The study received approval from the Istanbul University-Cerrahpasa Institutional Review Board on December 28, 2022 (Protocol number: 576635). Written informed consent was obtained from the patients’ legal representatives in accordance with the Declaration of Helsinki.
RESULTS
Study population
A total of 189 patients followed in the pediatric rheumatology outpatient clinic were included in the study. Of these, 94 (49.7%) had jSLE, 73 (38.6%) had FMF, and 22 (11.7%) had jSSc. Overall, 131 patients (69.3%) were female, and the proportion of females was significantly higher among jSLE patients (85.1%). The mean age at the last visit was 17.7 ± 4.8 years and was significantly lower in the FMF group (14.9 ± 3.6 years). Parental consanguinity was present in 44 patients (23.2%) and was more frequent among FMF patients (30.1%), although this difference did not reach statistical significance. In total, 7,034 individuals, including the patient cohort and their relatives, were screened for psoriasis. Among them, 738 were first-degree relatives (FDR), 2,380 were second-degree relatives (SDR), and 3,727 were third-degree relatives (TDR) (Table 1).
| FDR: First-degree relatives; FMF: Familial Mediterranean fever; jSLE: juvenile-onset systemic lupus erythematosus; jSSc: juvenile systemic sclerosis; SDR: Second-degree relatives; TDR: Third-degree relatives. | |||||
| Table 1. Demographic features in the study population | |||||
|
|
|
|
|
|
|
| Gender (female) |
|
|
|
|
|
| Age at last visit (year) |
|
|
|
|
|
| Consanguinity |
|
|
|
|
|
| FDR |
|
|
|
|
|
| SDR |
|
|
|
|
|
| TDR |
|
|
|
|
|
| Total |
|
|
|
|
|
Prevalence and recurrence rate of psoriasis in study groups and their relatives
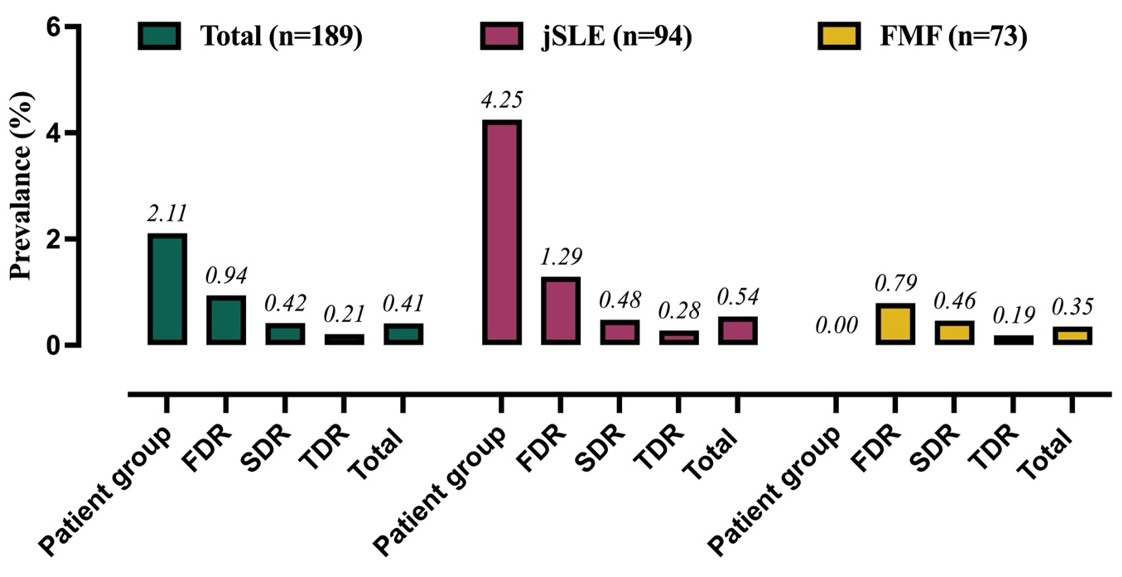
Psoriasis was detected in 4 of 189 patients (2.1%). Although the frequency was higher in the jSLE group (4.3%), no statistically significant difference was observed among the three disease groups (p = 0.23). The prevalence of psoriasis among first-, second-, and third-degree relatives was 7 (0.94%), 10 (0.42%), and 8 (0.21%), respectively, with no significant differences between these relative categories (p > 0.05). Overall, the prevalence of psoriasis in the entire study population, including patients and relatives, was 0.41%. The combined prevalence of psoriasis in jSLE patients and their relatives was 0.54%, which was significantly higher than in FMF (0.35%) and jSSc (0%) families (p = 0.034) (Table 2).
|
* Exact test (Fisher–Freeman–Halton) with Monte Carlo simulation FDR: First-degree relatives; FMF: Familial Mediterranean fever; jSLE: juvenile-onset systemic lupus erythematosus; jSSc: juvenile systemic sclerosis; SDR: Second-degree relatives; TDR: Third-degree relatives. |
|||||
| Table 2. Comparison of psoriasis prevalence among study patients and their relatives | |||||
|
|
|
|
|
|
|
| Patients |
|
|
|
|
|
| FDR |
|
|
|
|
|
| SDR |
|
|
|
|
|
| TDR |
|
|
|
|
|
| Total |
|
|
|
|
|
Since neither jSSc patients nor their relatives exhibited psoriasis, recurrence rates (λ) were calculated only for jSLE and FMF families. In jSLE, recurrence rates (λ) for the patient and their first-, second-, and third-degree relatives were 10.13, 3.07, 1.16, and 0.67, respectively. Although λ was highest in patients and FDR, comparison with an expected number of psoriasis cases based on general population prevalence did not show a statistically significant increase (p > 0.05) (Figure 1, Table 3). In FMF patients and their FDR, SDR, and TDR, recurrence rates (λ) were 0, 1.88, 1.11, and 0.45, respectively (Table 3).
|
# Fisher’s exact test assesses the difference in psoriasis rates between relatives and the general population using the same sample size. FDR: First-degree relatives; FMF: Familial Mediterranean fever; jSLE: juvenile-onset systemic lupus erythematosus; SDR: Second-degree relatives; TDR: Third-degree relatives. |
||||
| Table 3. Recurrence rate of psoriasis in patients with jSLE, FMF, and their relatives | ||||
|
|
|
|
|
|
| jSLE | ||||
| Affected relatives, no |
|
|
|
|
| Recurrence rate (λ) |
|
|
|
|
| p# |
|
|
|
|
| FMF | ||||
| Affected relatives, no |
|
|
|
|
| Recurrence rate (λ) |
|
|
|
|
| p# |
|
|
|
|
Comparison of clinical, laboratory, and activity features in jSLE patients, with and without psoriasis
Among the 94 jSLE patients, four had psoriasis, all of whom were female. Twenty patients with a personal or family history of psoriasis (21 psoriasis cases in total) were compared with 74 patients without a history of psoriasis to assess the impact on clinical and laboratory features. In the overall jSLE cohort, 80 patients (85.1%) were female. The mean ages at symptom onset and diagnosis were 11.5 ± 3.7 and 12.5 ± 3.3 years, respectively. The most common clinical manifestations were malar rash (74.4%), arthritis (50.0%), oral/nasal ulcers (43.6%), and photosensitivity (36.1%). Median SLEDAI-2K scores at diagnosis and at the last visit were 8 (5–12) and 2 (0–4), respectively. There were no statistically significant differences in clinical manifestations, laboratory parameters, or disease activity indices between patients with and without psoriasis (p > 0.05) (Table 4).
|
^Psoriasis cases among jSLE patients and their relatives Anti-Sm: anti-Smith antibody; Anti-dsDNA: anti-double-stranded DNA antibody; jSLE: juvenile-onset systemic lupus erythematosus; SLEDAI-2K: SLE Disease Activity Index 2000 |
||||
| Table 4. Comparison of clinical, laboratory, and activity features in jSLE patients and their relatives with and without psoriasis | ||||
|
|
|
|
|
|
| Gender (female) |
|
|
|
|
| Symptom onset age (year) |
|
|
|
|
| Diagnosis age (year) |
|
|
|
|
| Acute or subacute cutaneous lupus |
|
|
|
|
| Chronic cutaneous lupus |
|
|
|
|
| Malar rash |
|
|
|
|
| Discoid rash |
|
|
|
|
| Photosensitivity |
|
|
|
|
| Alopecia |
|
|
|
|
| Oral/nasal ulcers |
|
|
|
|
| Arthritis |
|
|
|
|
| Neuropsychiatric involvement |
|
|
|
|
| Hematological involvement |
|
|
|
|
| Proteinuria |
|
|
|
|
| Anti-dsDNA positivity |
|
|
|
|
| Anti-Sm positivity |
|
|
|
|
| SLEDAI-2K (at diagnosis) |
|
|
|
|
| SLEDAI-2K (at last visit) |
|
|
|
|
DISCUSSION
This study is the first to investigate the risk of psoriasis among patients with jSLE and their relatives and to estimate the familial transmission of psoriasis across pediatric rheumatic diseases using a population-based prevalence reference. We observed that the recurrence rate of psoriasis in jSLE patients (10.1) and their first-degree relatives (3.0) was higher than in individuals with FMF or jSSc and their relatives. Although the difference between patients and their relatives with psoriasis was not statistically significant, we demonstrated that the combined group of jSLE patients and their relatives had a significantly higher prevalence of psoriasis compared with the combined FMF and jSSc groups and their relatives. In this study, a positive family history of psoriasis was not associated with more severe jSLE. Clinical, laboratory, and disease activity characteristics in our jSLE cohort were comparable to those reported in previous published cohorts.12-15
The coexistence of psoriasis and jSLE is very rare, and only a limited number of such cases have been reported in the literature.16 In the study by Walters et al., including 62 patients with jSLE, psoriasis was reported in the families of four (6%) patients, and in three of them, the affected relative was FDR.17 Tselios et al. identified psoriasis in 3.46% of 832 adult-onset SLE (aSLE) patients; the prevalence of psoriasis in this lupus cohort was approximately twice that of the general Canadian population.18 Similar to our findings, Walhelm et al. evaluated 351 aSLE patients and found psoriasis in 12 (3.4%), with no significant differences in clinical, laboratory, or SLEDAI-2K scores between those with and without psoriasis. Overall, clinical and immunological features were similar in both groups.19
In a large population-based study, Huang et al. demonstrated clear familial aggregation of psoriasis, reporting a 5.5-fold and 2.5-fold increased risk of psoriasis among individuals with affected FDR and SDR, respectively, compared with the general population, indicating a relationship between genetic proximity and psoriasis risk. Notably, individuals with a family history of psoriasis also had higher risks of rheumatoid arthritis, primary Sjögren’s syndrome, SLE, and SSc, supporting shared autoimmune susceptibility.20 Similarly, Barut et al. reported a markedly higher frequency of psoriasis family history in children with FMF compared with healthy controls and patients with juvenile idiopathic arthritis.21 In another study specifically addressing familial aggregation of SLE, the risks of SLE and other autoimmune diseases (mainly primary Sjögren’s syndrome, SSc, and myasthenia gravis) were elevated among relatives of SLE patients, and the heritability of SLE was estimated at 43.9%, underscoring the importance of considering familial aggregation and heritability when counseling affected families.22 Consistent with this, Sinicato et al. further documented familial aggregation by demonstrating differences in recurrence risk ratios by degree of relatedness between juvenile-onset and adult-onset SLE within the same population, suggesting a higher genetic load and a more polygenic and epistatic pattern of inheritance in jSLE. Together, these findings support the notion that the genetic architecture of SLE may differ according to age at disease onset.23
Genome-wide association studies (GWASs) have identified numerous genetic risk loci for many autoimmune diseases. Among these loci, several are shared by psoriasis and SLE, including PTPN22, STAT4, TNIP1, NFKBIA, and IL28RA.24 NFKBIA encodes the inhibitory protein IκBα, which restrains NF-κB dimers in the cytoplasm and thereby suppresses their activation. Chronic activation of the NF-κB pathway enhances pro-inflammatory gene expression in the pathogenesis of both SLE and psoriasis, whereas dysfunction of NFKBIA/IκBα may fail to adequately constrain this pathway, thereby increasing disease susceptibility and amplifying inflammatory responses.25 In a previous study, serum NF-κB levels in patients with jSLE showed a trend toward higher levels than in healthy controls.26
This study has several limitations. First, the cross-sectional design precludes any inference of causality between family history of psoriasis and the occurrence or clinical features of jSLE, jSSc, or FMF. Second, the study was conducted in a single tertiary referral center, and the control group was hospital-based, potentially limiting the generalizability of the results to the broader pediatric population. The relatively low number of psoriasis cases in our cohort, including the absence of psoriasis in the jSSc group, may have reduced the statistical power of some between-group comparisons; therefore, these findings should be interpreted with caution. Finally, we were not able to evaluate the impact of psoriasis subtype, severity, or treatment on the observed relationships, which may have provided further insight into potential shared genetic or immunologic mechanisms.
In conclusion, our findings indicate that a positive family history of psoriasis is more common in jSLE than in FMF or jSSc, supporting the hypothesis of a shared genetic background between psoriasis and jSLE. Although our results should be interpreted in light of the study limitations, they highlight the importance of systematically asking about familial psoriasis when evaluating children with SLE and related conditions. Larger, prospective, population-based studies are needed to confirm these associations and to clarify the underlying genetic and immunological mechanisms.
Ethical approval
This study was approved by the Istanbul University- Cerrahpasa, Cerrahpasa Faculty of Medicine Institutional Review Board (Date: 28.12.2022, Decision/Protocol No: 576635). Informed consent was obtained from all participants involved in this study.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declare that this study received no funding.
Generative AI statement
The authors declare that no generative AI or AI-assisted technologies were used in the writing or preparation of this study.
References
- Bieber K, Hundt JE, Yu X, et al. Autoimmune pre-disease. Autoimmun Rev. 2023;22:103236. https://doi.org/10.1016/j.autrev.2022.103236
- Fijałkowska A, Wojtania J, Woźniacka A, Robak E. Psoriasis and lupus erythematosus-similarities and differences between two autoimmune diseases. J Clin Med. 2024;13:4361. https://doi.org/10.3390/jcm13154361
- Cakır N, Pamuk ÖN, Derviş E, et al. The prevalences of some rheumatic diseases in western Turkey: Havsa study. Rheumatol Int. 2012;32:895-908. https://doi.org/10.1007/s00296-010-1699-4
- Smith EMD, Lythgoe H, Hedrich CM. Current views on lupus in children. Curr Opin Rheumatol. 2023;35:68-81. https://doi.org/10.1097/BOR.0000000000000913
- Avar-Aydın PÖ, Brunner HI. Revisiting childhood-onset systemic lupus erythematosus. Turk Arch Pediatr. 2024;59:336-44. https://doi.org/10.5152/TurkArchPediatr.2024.24097
- Setoue DN, Pitta AC, Fiorot FJ, et al. Symptomatic polyautoimmunity at diagnosis of 1463 childhood-onset lupus: a Brazilian multicenter study. Autoimmun Rev. 2018;17:836-9. https://doi.org/10.1016/j.autrev.2018.03.009
- Konte EK, Karakas H, Akay N, et al. Evaluation of thyroid dysfunction in childhood-onset systemic lupus erythematosus: risk factors for hashimoto’s thyroiditis. Lupus. 2024;33:1235-41. https://doi.org/10.1177/09612033241272964
- Huang CM, Yang YH, Chiang BL. Different familial association patterns of autoimmune diseases between juvenile-onset systemic lupus erythematosus and juvenile rheumatoid arthritis. J Microbiol Immunol Infect. 2004;37:88-94.
- Gattorno M, Hofer M, Federici S, et al. Classification criteria for autoinflammatory recurrent fevers. Ann Rheum Dis. 2019;78:1025-32. https://doi.org/10.1136/annrheumdis-2019-215048
- Aringer M, Costenbader K, Daikh D, et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Ann Rheum Dis. 2019;78:1151-9. https://doi.org/10.1136/annrheumdis-2018-214819
- Zulian F, Woo P, Athreya BH, et al. The Pediatric Rheumatology European Society/American College of Rheumatology/European League Against Rheumatism provisional classification criteria for juvenile systemic sclerosis. Arthritis Care Res. 2007;57:203-12. https://doi.org/10.1002/art.22551
- Eravsar A, Demirbas KC, Aslan E, et al. Predictors of damage accrual in childhood-onset SLE: a retrospective analysis from a tertiary lupus centre in Türkiye. Lupus Sci Med. 2025;12:e001634. https://doi.org/10.1136/lupus-2025-001634
- Sahin S, Adrovic A, Barut K, et al. Juvenile systemic lupus erythematosus in Turkey: demographic, clinical and laboratory features with disease activity and outcome. Lupus. 2018;27:514-9. https://doi.org/10.1177/0961203317747717
- Aslan E, Sahin S, Bektas S, et al. The performance of the 2019 EULAR/ACR classification criteria in childhood-onset systemic lupus erythematosus. Lupus. 2025;34:511-8. https://doi.org/10.1177/09612033251325321
- Kavrul Kayaalp G, Esencan D, Guliyeva V, et al. Childhood-onset systemic lupus erythematosus: A descriptive and comparative study of clinical, laboratory, and treatment characteristics in two populations. Lupus. 2024;33:1130-8. https://doi.org/10.1177/09612033241265975
- Dybowska-Gołota I, Owczarczyk-Saczonek A, Krajewska-Włodarczyk M, Żuber Z. Psoriasis and systemic lupus erythematosus in children - literature review based on case report. Reumatologia. 2020;58:48-55. https://doi.org/10.5114/reum.2020.93516
- Walters HM, Pan N, Moorthy LN, Ward MJ, Peterson MG, Lehman TJ. Patterns and influence of familial autoimmunity in pediatric systemic lupus erythematosus. Pediatr Rheumatol Online J. 2012;10:22. https://doi.org/10.1186/1546-0096-10-22
- Tselios K, Yap KSY, Pakchotanon R, et al. Psoriasis in systemic lupus erythematosus: a single-center experience. Clin Rheumatol. 2017;36:879-84. https://doi.org/10.1007/s10067-017-3566-0
- Walhelm T, Parodis I, Enerbäck C, Arkema E, Sjöwall C. Comorbid psoriasis in systemic lupus erythematosus: a cohort study from a tertiary referral centre and the National Patient Register in Sweden. Lupus Sci Med. 2025;12:e001504. https://doi.org/10.1136/lupus-2025-001504
- Huang YH, Kuo CF, Huang LH, Hsieh MY. Familial aggregation of psoriasis and co-aggregation of autoimmune diseases in affected families. J Clin Med. 2019;8:115. https://doi.org/10.3390/jcm8010115
- Barut K, Guler M, Sezen M, Kasapçopur O. Increased frequency of psoriasis in the families of children with familial Mediterranean fever. Clin Exp Rheumatol. 2014;12(Suppl 1):258.
- Kuo CF, Grainge MJ, Valdes AM, et al. Familial aggregation of systemic lupus erythematosus and coaggregation of autoimmune diseases in affected families. JAMA Intern Med. 2015;175:1518-26. https://doi.org/10.1001/jamainternmed.2015.3528
- Sinicato NA, de Oliveira L, Lapa A, et al. Familial aggregation of childhood- and adulthood-onset systemic lupus erythematosus. Arthritis Care Res (Hoboken). 2020;72:1147-51. https://doi.org/10.1002/acr.23931
- Li Y, Cheng H, Zuo XB, et al. Association analyses identifying two common susceptibility loci shared by psoriasis and systemic lupus erythematosus in the Chinese Han population. J Med Genet. 2013;50:812-8. https://doi.org/10.1136/jmedgenet-2013-101787
- Yu H, Lin L, Zhang Z, Zhang H, Hu H. Targeting NF-κB pathway for the therapy of diseases: mechanism and clinical study. Signal Transduct Target Ther. 2020;5:209. https://doi.org/10.1038/s41392-020-00312-6
- Durmus S, Sahin S, Adrovic A, et al. Interplay of NF-κB and PPAR-γ transcription factors in patients with juvenile systemic lupus erythematosus. Lupus Sci Med. 2025;12:e001263. https://doi.org/10.1136/lupus-2024-001263
Copyright and license
Copyright © 2026 The author(s). This is an open-access article published by Aydın Pediatric Society under the terms of the Creative Commons Attribution License (CC BY) which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.
