
Abstract
Objective: Behçet’s disease (BD) is a variable-vessel vasculitis with multisystemic involvement. Although cytokine dysregulation has been extensively investigated, data on angiogenic and vascular marker profiles remain limited in pediatric BD. This exploratory study aimed to characterize circulating vascular and inflammatory mediator profiles in pediatric BD, compare them with deficiency of adenosine deaminase 2 (DADA2) and polyarteritis nodosa (PAN). It further aimed to assess whether these markers were associated with vascular or central nervous system (CNS) involvement in BD.
Methods: Serum samples from BD (n=34), DADA2 (n=20), PAN (n=10), and healthy controls (n=8) were analyzed for thirteen vascular and inflammatory markers (TIE1, TIE2, FLT1, sT2, RAGE, CD40L, LIGHT, PlGF, TNF-α, IL-6, IL-10, IL-18, MCP-1) using a multiplex bead-based immunoassay. Statistical analyses included Kruskal–Wallis and Mann–Whitney U tests for group comparisons, logistic and linear regression for associations with clinical features, and Spearman correlation to explore interrelations among markers.
Results: TIE2 levels were significantly reduced in BD compared with healthy controls (p=0.010). DADA2 patients exhibited a distinct angiogenic–inflammatory profile, with significantly elevated levels of TIE1, TIE2, FLT1, TNF-α, IL-10, IL-18, and MCP-1 (all p<0.010) compared with both BD and PAN. None of the circulating markers independently predicted vascular or CNS involvement in BD. Strong positive correlations among angiogenic mediators (FLT1, PlGF, LIGHT) suggested a coordinated vascular signaling pattern, particularly in DADA2.
Conclusion: Although individual circulating mediators showed limited discriminatory performance across vasculitis subtypes, DADA2 displayed a more distinct vascular-inflammatory profile characterized by TNF-α- and TIE2-related pathways. In pediatric BD, reduced TIE2 may reflect altered endothelial homeostasis, although this finding should be interpreted cautiously. These results support the need for integrated multi-marker approaches and longitudinal sampling to better define vascular-immune phenotypes in pediatric vasculitis.
Keywords: Behçet’s disease, adenosine deaminase deficiency, polyarteritis nodosa, vasculitis
INTRODUCTION
Behçet’s disease (BD) is a variable-vessel, multisystemic vasculitis characterized by recurrent mucocutaneous ulcers, ocular inflammation, vascular thrombosis, and neurological involvement. Although the underlying mechanisms remain incompletely understood, BD is increasingly recognized as a disorder of immune-mediated vascular inflammation, in which dysregulated cytokine networks and endothelial injury play central roles. Numerous studies have demonstrated varying results with elevations of Th1 and Th17-related cytokines, including IL-6, IL-8, TNF-α, IL-17, and IFN-γ, during disease flares.1,2
Beyond these classical cytokines, emerging evidence points to the importance of endothelial dysfunction and aberrant angiogenic signaling in BD pathogenesis. Biomolecules such as angiopoietin–TIE receptor pathway components (TIE1, TIE2), soluble fms-like tyrosine kinase-1 (FLT1), placental growth factor (PlGF), and receptor for advanced glycation end-products (RAGE) have been implicated in vascular homeostasis and inflammation. However, their role in BD, particularly in pediatric populations, remains largely unexplored. Most studies to date have focused on adult cohorts and have primarily addressed proinflammatory cytokines, leaving the vascular and endothelial dimensions of pediatric BD insufficiently characterized.3-5
Comparative analysis with other vasculitides that share overlapping vascular features may help identify shared and distinct vascular-inflammatory patterns. Deficiency of adenosine deaminase 2 (DADA2) represents a monogenic vasculitis characterized by systemic inflammation, endothelial injury, and TNF-driven vascular pathology, often mimicking polyarteritis nodosa (PAN).6,7 Idiopathic PAN involves necrotizing arteritis of medium-sized vessels but lacks the prominent mucocutaneous and thrombotic features of BD. Studying these entities in parallel may provide insight into both overlapping and divergent angiogenic-inflammatory pathways across pediatric vasculitis.
The present study was designed as an exploratory analysis to characterize circulating vascular and inflammatory mediator profiles (including TIE1, TIE2, FLT1, soluble ST2 [sT2], receptor for advanced glycation end-products [RAGE], CD40 ligand [CD40L], lymphotoxin-like inducible protein [LIGHT], placental growth factor [PlGF], TNF-α, IL-6, IL-10, IL-18, and monocyte chemoattractant protein-1 [MCP-1]) in pediatric BD and to compare them with those observed in DADA2, PAN, and healthy controls. It further aimed to evaluate whether these markers were associated with vascular or central nervous system (CNS) involvement in BD.
MATERIALS and METHODS
Study population
This cross-sectional study included pediatric patients followed at the Pediatric Rheumatology Department of Hacettepe University, Ankara. Serum samples were collected from four groups: patients with BD (n = 34), DADA2 (n = 20), PAN (n = 10), and age-matched healthy controls (HC, n = 8). All participants were of Turkish origin.
BD was diagnosed according to the Pediatric Behçet’s Disease (PEDBD) classification criteria. DADA2 was confirmed by biallelic pathogenic variants in ADA2 and/or decreased ADA2 enzyme activity (<5% of normal). PAN patients fulfilled the Ankara 2008 criteria. Genetic screening for ADA2 variants was not routinely performed in PAN patients because no clinical features suggestive of DADA2 were present.
Blood samples were obtained during clinically stable visits, at least four weeks after the last disease flare. Treatment exposure at the time of sampling was also recorded for all participants. All participants were free of acute infection, metabolic, or neoplastic disease at the time of sampling. This study was approved by the Hacettepe University Ethics Commission (Approval No: GO 19/275). Written informed consent was obtained from all participants or their legal guardians prior to inclusion.
Sample collection and mediator profile analysis
Peripheral venous blood samples were collected during routine follow-up visits using serum separator tubes and centrifuged at 4000 rpm for 10 minutes. The sera were aliquoted and stored at –80°C until analysis. Serum levels of angiogenic and inflammatory analytes (TIE2, TIE1, FLT1, sT2, RAGE, CD40L, LIGHT, PlGF, TNF-α, IL-6, IL-10, IL-18, and MCP-1) were measured using a multiplex bead-based immunoassay (LEGENDplex™ HU Vascular Inflammation Panel 2 (13-plex); Cat#740966, BioLegend, San Diego, CA, USA). Assays were performed according to the manufacturer’s instructions, and data acquisition was conducted using a Luminex® platform. All samples were tested in duplicate within the same assay run to minimize inter-assay variability.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics version 26.0 (Armonk, NY, USA) and GraphPad Prism 10.0. Continuous variables were summarized as mean ± standard deviation (SD) or median (interquartile range, IQR), depending on the data distribution, as assessed by the Shapiro–Wilk test. Categorical variables were expressed as frequencies and percentages. Group comparisons were conducted using the Kruskal–Wallis test followed by Dunn–Bonferroni post-hoc correction for non-normally distributed data and one-way ANOVA with Tukey correction for normally distributed data. Correlations among markers were evaluated using Spearman’s rank correlation coefficient (ρ).
Multiple linear regression analyses were applied to explore associations between marker levels and disease duration, while binary logistic regression was used to identify potential predictors of vascular or CNS involvement in BD. Variables with p < 0.100 in univariate analysis or with biological relevance were entered into multivariable models. Model adequacy was assessed by the Hosmer–Lemeshow goodness-of-fit test, R², and adjusted R². All tests were two-tailed, and p < 0.05 was considered statistically significant.
RESULTS
Study population
A total of 72 serum samples were collected and analyzed from 72 consecutive individuals, including patients diagnosed with BD (n=34, 47.2%), DADA2 (n=20, 27.8%), PAN (n=10, 13.9%), and HC (n=8, 11.1%). The mean age of participants was 10.66 ± 4.42 years, and 44.4% (n=32) were male. Among BD patients, the mean age at diagnosis was 11.7 ± 3.2 years, and the mean disease duration at the time of sampling was 82.6 ± 48.2 days. Clinical characteristics of BD patients are summarized in Table 1. Vascular involvement was present in 7 (20.6%) BD patients, and CNS involvement in 5 (14.7%). All DADA2 patients had documented vascular disease. At the time of sampling, treatment exposure differed across groups. In the BD group, 10/34 patients were untreated, while the remaining patients were receiving colchicine (21/34), corticosteroids (5/34), azathioprine (4/34), adalimumab (2/34), infliximab (1/34), or cyclophosphamide (1/34), alone or in combination. All patients with DADA2 were receiving anti-TNF therapy, whereas all PAN patients and healthy controls were untreated.
| SD, standard deviation; IQR, interquartile range; WBC, white blood cell count; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; HLA, human leukocyte antigen. | ||
| Table 1. Clinical and laboratory characteristics of patients with Behçet’s disease (n = 34) | ||
| Category |
|
|
| Demographic |
|
|
|
|
|
|
|
|
|
|
| Clinical |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Laboratory |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
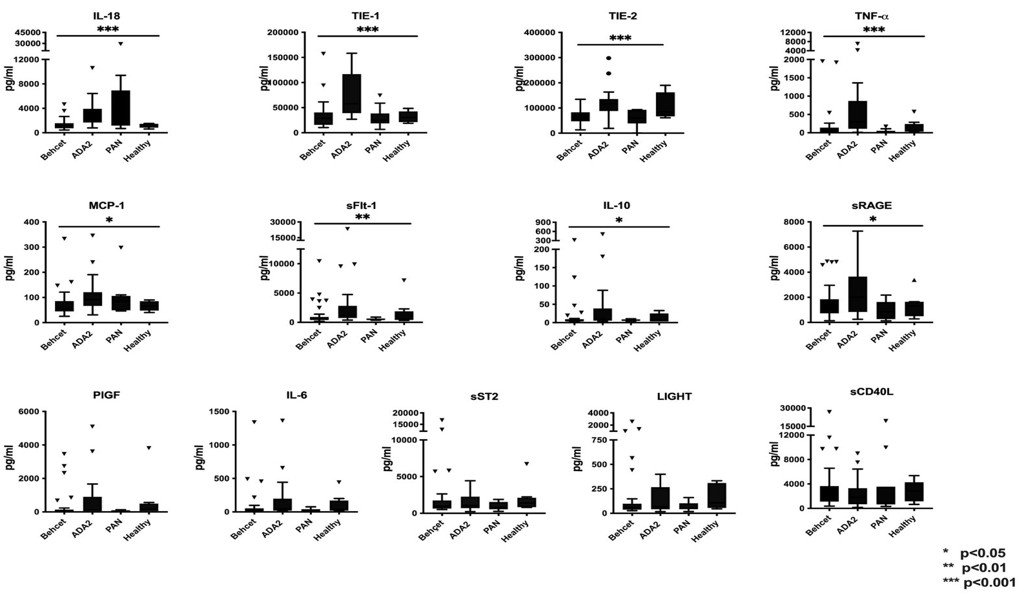
Mediator profiles across disease groups
Comparative analysis revealed distinct patterns of vascular and inflammatory mediators across the four study groups (Figure 1). In BD, TIE2 levels were significantly lower than in healthy controls (p = 0.010). In contrast, patients with DADA2 exhibited elevated levels of angiogenic and inflammatory markers, including TIE1, TIE2, FLT1, TNF-α, IL-18, IL-10, and MCP-1, compared with both PAN and BD (all p < 0.001). FLT1 levels in DADA2 were also higher than in healthy controls (p = 0.042). PAN patients showed intermediate values, with IL-18 significantly higher than in BD (p = 0.003) but lower than in DADA2.
Despite group-level differences, receiver operating characteristic (ROC) analyses indicated limited diagnostic performance of individual circulating markers; all area under the curve (AUC) values were < 0.7.
Multiple linear regression analysis including all markers as predictors of disease duration in BD yielded no significant associations (R² = 0.23, adjusted R² = –0.44). Similarly, in logistic regression models, none of the evaluated markers independently predicted vascular (χ² = 12.6, p = 0.082) or CNS involvement (all p > 0.050).
Spearman correlation analyses demonstrated strong positive relationships among several angiogenic and inflammatory markers: sT2 strongly correlated with LIGHT (ρ = 0.776, p < 0.001), PlGF (ρ = 0.681, p < 0.001), and FLT1 (ρ = 0.576, p < 0.001). FLT1 correlated with PlGF (ρ = 0.843), LIGHT (ρ = 0.797), and IL-6 (ρ = 0.617). TIE2 moderately correlated with FLT1 (ρ = 0.568) and PlGF (ρ = 0.523). These relationships were mostly pronounced in DADA2. These findings are illustrated in Figure 1.
DISCUSSION
In this study, we examined a panel of vascular and inflammatory markers in pediatric patients with BD and compared their profiles with those of patients with DADA2 and PAN, as well as healthy controls. This exploratory analysis showed that although several intergroup differences were present, individual circulating markers had limited discriminatory utility across pediatric vasculitis subtypes. Nevertheless, the observed patterns provide insight into the vascular-inflammatory milieu of these conditions, particularly in DADA2.
Patients with DADA2 exhibited the most pronounced angiogenic-inflammatory alterations in our cohort, with significantly elevated TIE1, TIE2, FLT1, TNF-α, IL-18, IL-10, and MCP-1 compared with both BD and PAN.
These findings are consistent with previous reports highlighting endothelial dysregulation and TNF-driven vascular inflammation in DADA2.6
TIE2, a receptor tyrosine kinase activated by angiopoietin-1 and -2, plays a critical role in endothelial homeostasis, vascular remodeling, and inflammatory signaling.1 Consistent with this, Kaya Akca et al. reported increased levels of TIE1, TIE2, and TNF-α in pediatric DADA2 patients compared to PAN, proposing that these markers reflect key differences in immune-mediated vascular injury despite overlapping clinical features.6 The consistently high TNF-α levels in DADA2 align with its known therapeutic relevance and further highlight the role of TNF-driven endothelial inflammation. Taken together, our results support the notion that the angiogenic and cytokine milieu—particularly involving TIE2 and TNF-α—may serve as potential mechanistic indicators or biomarkers in DADA2, distinct from other forms of systemic vasculitis. Notably, all DADA2 patients were receiving anti-TNF therapy at the time of sampling. Therefore, the observed profile should not be interpreted as entirely treatment-independent, although the persistence of this pattern despite anti-TNF exposure may still reflect ongoing disease-related vascular immune activation.
In contrast, patients with BD showed a more heterogeneous cytokine profile, with overall lower levels of TNF-α and IL-18, and no significant elevation of angiogenic markers compared to controls, except for decreased TIE2 levels. This contrasts with previous reports suggesting elevated IL-182 and TNF-α levels in active BD.4 Several factors may explain the relatively modest inflammatory signal observed in BD. First, samples were collected during clinically stable follow-up visits rather than active inflammatory attacks, which may have attenuated cytokine elevations. Second, treatment exposure was common in the BD group: only 10 of 34 patients were untreated, while the remaining patients were receiving colchicine, corticosteroids, azathioprine, or biologic agents. These factors may partly explain the comparatively low levels of TNF-α and IL-18 in BD and the overlap observed with other disease groups.
An important finding of our study is that individual circulating markers showed limited discriminatory performance across pediatric vasculitis subtypes. All ROC AUC values remained below 0.7, indicating that no single marker provided clinically useful discrimination among BD, DADA2, and PAN in this cohort. Although negative, this finding is clinically relevant because it argues against overinterpretation of isolated serum measurements and suggests that single-marker approaches are insufficient for disease classification in pediatric vasculitis.5
We also did not identify significant associations between circulating markers and vascular or CNS involvement in BD. This contrasts with some adult studies reporting elevated cytokine levels in active or organ-specific disease; however, our findings should be interpreted in the context of important methodological constraints.3,8 In particular, the number of BD patients with vascular (n = 7) and CNS involvement (n = 5) was small, limiting statistical power and increasing the risk of unstable estimates in regression analyses. Accordingly, these subgroup analyses should be regarded as exploratory.
This study has several important limitations. First, the sample size was modest, particularly in the BD subgroups with vascular and CNS involvement. Second, the cross-sectional design precluded assessment of longitudinal changes in marker levels over time. Third, samples were collected during clinically stable visits rather than active flares, which may have limited the detection of disease activity-related signals. Fourth, treatment exposure differed substantially across groups, with heterogeneous ongoing therapy in BD, universal anti-TNF use in DADA2, and no treatment in PAN, potentially confounding intergroup comparisons. Finally, reliance on peripheral blood measurements may not fully capture tissue-level or organ-specific vascular inflammation.
CONCLUSION
In conclusion, our findings suggest that single circulating markers are of limited value for distinguishing pediatric BD from other vasculitides or for predicting vascular and CNS involvement in BD. In contrast, DADA2 demonstrated a more distinct vascular-inflammatory pattern characterized by coordinated angiogenic and TNF-related signals. These observations support the need for larger, longitudinal, treatment-stratified studies and integrated multi-marker approaches to better define clinically meaningful vascular-immune phenotypes in pediatric vasculitis.
Ethical approval
This study was approved by the Hacettepe University Ethics Committee (approval date 25.09.2019, number: GO 19/275). Informed consent was obtained from all participants involved in this study.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declare that this study received no funding.
Generative AI statement
The authors declare that no generative AI or AI-assisted technologies were used in the writing or preparation of this study.
References
- Mendoza-Pinto C, García-Carrasco M, Jiménez-Hernández M, et al. Etiopathogenesis of Behcet’s disease. Autoimmun Rev. 2010;9:241-5. https://doi.org/10.1016/j.autrev.2009.10.005
- Yamagata T, Skepner J, Yang J. Targeting Th17 effector cytokines for the treatment of autoimmune diseases. Arch Immunol Ther Exp (Warsz). 2015;63:405-14. https://doi.org/10.1007/s00005-015-0362-x
- Hamzaoui K, Hamzaoui A, Guemira F, Bessioud M, Hamza M, Ayed K. Cytokine profile in Behçet’s disease patients. Relationship with disease activity. Scand J Rheumatol. 2002;31:205-10. https://doi.org/10.1080/030097402320318387
- Düzgün N, Ayaşlioğlu E, Tutkak H, Aydintuğ OT. Cytokine inhibitors: soluble tumor necrosis factor receptor 1 and interleukin-1 receptor antagonist in Behçet’s disease. Rheumatol Int. 2005;25:1-5. https://doi.org/10.1007/s00296-003-0400-6
- Cantarini L, Pucino V, Vitale A, et al. Immunometabolic biomarkers of inflammation in Behçet’s disease: relationship with epidemiological profile, disease activity and therapeutic regimens. Clin Exp Immunol. 2016;184:197-207. https://doi.org/10.1111/cei.12768
- Kaya Akca U, Sag E, Unal S, Kasap Cuceoglu M, Bilginer Y, Ozen S. The role of vascular inflammation markers in deficiency of adenosine deaminase 2. Semin Arthritis Rheum. 2021;51:839-44. https://doi.org/10.1016/j.semarthrit.2021.04.013
- García S, Krausz S, Ambarus CA, et al. Tie2 signaling cooperates with TNF to promote the pro-inflammatory activation of human macrophages independently of macrophage functional phenotype. PLoS One. 2014;9:e82088. https://doi.org/10.1371/journal.pone.0082088
- Hamzaoui A, Ghraïri H, Ammar J, Zekri S, Guemira F, Hamzaoui K. IL-18 mRNA expression and IFN-gamma induction in bronchoalveolar lavage from Behçet’s disease. Clin Exp Rheumatol. 2003;21(4 Suppl 30):S8-14.
Copyright and license
Copyright © 2026 The author(s). This is an open-access article published by Aydın Pediatric Society under the terms of the Creative Commons Attribution License (CC BY) which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.
