Abstract
Skin rashes and lesions are among the most common health concerns in pediatric patients, yet access to pediatric dermatologists remains limited. This shortage contributes to delays in clinical diagnoses, suboptimal treatment, and reduced quality of life for affected patients. Artificial intelligence (AI), particularly image-based diagnostic and decision-support tools, offers a promising approach to augment care delivery in regions where specialist access is scarce.
AI has the potential to improve diagnostic accuracy and enhance triage for common pediatric skin conditions. By assisting clinicians in identifying disorders and recommending evidence-based management pathways, AI can reduce the time to intervention. Recent studies have demonstrated that AI can achieve diagnostic accuracy comparable to that of specialists and improve clinician performance when used as a support tool. To ensure these benefits are equitably distributed, however, AI tools must be designed with attention to social determinants of health, including disparities in digital access, bias in algorithm training, and the need for cultural competence.
This review examines the current applications of AI in pediatric dermatology, with a focus on its role in rural and primary care settings. It also explores how AI intersects with the social determinants of health and the psychosocial well-being of children, including stigma, mental health, and quality of life. Equitable design and careful implementation will determine whether AI can effectively assist pediatric dermatologic care or exacerbate existing disparities.
Our analysis draws on peer-reviewed literature and publicly available AI tools from PubMed and Google Scholar, using Boolean operations.
Keywords: Artificial intelligence (AI), pediatric dermatology, social determinants of health, quality of life, underserved communities, health equity
INTRODUCTION
Pediatric skin conditions, such as atopic dermatitis, acne, and warts, are a frequent complaint in primary care visits, accounting for up to 30% of encounters in some studies. Despite this high demand, access to pediatric dermatologists remains scarce across the United States.1 Contributing factors include a small number of training programs, financial disincentives, geographic maldistribution, and long wait times. Pediatric dermatology only became a formally recognized subspecialty in 2004 and has since struggled to grow due to both workforce shortages and economic constraints. Many pediatric residents who develop an interest in dermatology find they are not competitive for dermatology residency. In contrast, dermatology residents are often discouraged from pursuing pediatric subspecialization due to lower reimbursement compared to fields like cosmetic dermatology.2
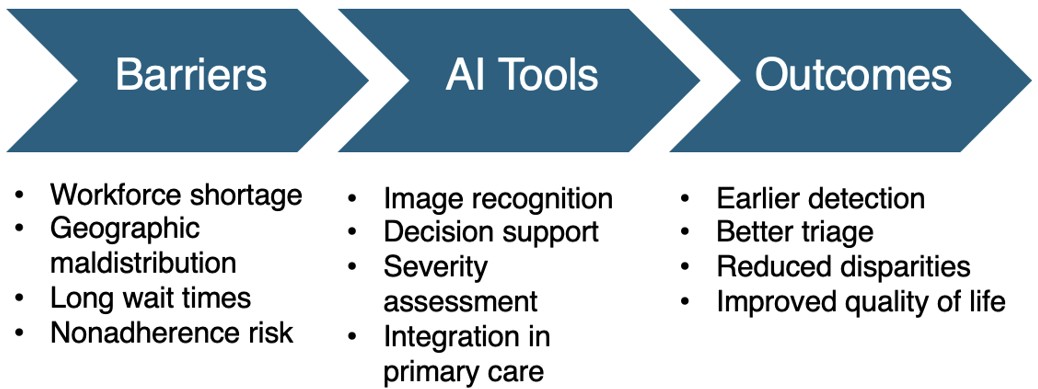
Structural barriers further compound this shortage. Insurance restrictions and long travel distances disproportionately impact underserved communities, particularly Medicaid patients. While many dermatologists are listed as Medicaid providers, 44% decline to accept new pediatric patients.3 Pediatric dermatologists also tend to cluster in urban areas, leaving patients in rural areas with longer travel times and longer wait times. For example, the average clinic wait time exceeds six weeks, with 25% patients waiting over 10 weeks.4 Families traveling more than 20 miles were over seven times more likely to be nonadherent to treatment plans, resulting in worse health outcomes.5 These systemic barriers highlight the urgent need for innovative strategies to expand access to dermatologic care for children, especially in underserved communities (Figure 1).
MATERIALS AND METHODS
For this review, we searched the electronic PubMed/Medline and Google Scholar databases for peer-reviewed articles on AI and pediatric dermatology, preferably published within the last 5 years. The keywords used were: “Artificial intelligence (AI), pediatric dermatology, social determinants of health, quality of life, underserved communities, health equity.” AND, OR, and NOT Boolean operators were used to refine searches by combining or excluding keywords. As a result, a total of 45 articles were identified. The aim was to synthesize existing evidence and offer critical analysis and insights to inform providers. The papers were evaluated based on their titles, abstracts, and complete texts, with the primary inclusion criteria being the description of AI use in dermatology. The most important exclusion criterion was that the article addressed diseases other than AI use in skin conditions. Papers that were not written in the English language were also excluded. An independent search was performed by all authors in the mentioned databases. Disagreements in the selection of literature were resolved through discussion and consensus among authors. Inter-rater agreement was not formally quantified, but it was achieved before inclusion. The included articles met all inclusion and exclusion criteria, including those written specifically for children under 18 years of age. One author reviewed the reference lists of each retrieved article to identify other articles that could be selected per the eligibility criteria. The main author began collecting data by reviewing the literature in January 2025. However, the final review of data sources was conducted in June 2025 by both authors. The review included 20 articles after the final evaluation. Please refer to Table 1 for the main article conclusions.
| Table 1. Summary of literature review | |||
| Article | Authors | Conclusion | |
| 1 | Pediatric dermatology: past, present, and future | Prindaville B, Antaya RJ, Siegfried EC. | Pediatric dermatology workforce shortage is due to limited training pathways and geographic maldistribution |
| 2 | Geographic distribution and characteristics of the pediatric dermatology workforce in the United States | Sinha S, Lin G, Zubkov M, Wu R, Feng H. | Majority of the pediatric dermatology workforce is clustered in urban regions |
| 3 | Pediatric access to dermatologists: Medicaid versus private insurance | Chaudhry SB, Armbrecht ES, Shin Y, et al. | Pediatric patients with Medicaid have reduced access to dermatologists |
| 4 | Pediatric dermatology workforce in the United States | Prindaville B, Horii KA, Siegfried EC, Brandling-Bennett H. | Geographic maldistribution of pediatric dermatologists in the US causes long wait times and further care shortages |
| 5 | Distance traveled affects adherence to treatment and follow-up plans for patients with infantile hemangioma | Desrosiers AS, Ibrahim JM, Jacks SK. | Greater travel distance to a pediatric dermatologist is associated with lower treatment adherence and reduced follow-up attendance |
| 6 | Artificial intelligence in healthcare: An essential guide for health leaders | Chen M, Decary M. | AI can augment clinician decision-making, improve efficiency, and support care delivery when integrated into clinical workflows |
| 7 | Artificial intelligence and health inequities in primary care: a systematic scoping review and framework. | D’Elia A, Gabbay M, Rodgers S, et al. | AI can improve primary care but may exacerbate health inequities if not implemented thoughtfully |
| 8 | Development and Assessment of an Artificial Intelligence-Based Tool for Skin Condition Diagnosis by Primary Care Physicians and Nurse Practitioners in Teledermatology Practices | Jain A, Way D, Gupta V, et al. | AI diagnostic tool improved clinician accuracy and agreement with dermatologists in teledermatology |
| 9 | Infantile hemangioma. Part 1: Epidemiology, pathogenesis, clinical presentation and assessment | Rodríguez Bandera AI, Sebaratnam DF, Wargon O, Wong LF. | Review of infantile hemangioma and the importance of early recognition and assessment |
| 10 | Development of an artificial intelligence algorithm for the diagnosis of infantile hemangiomas | Zhang AJ, Lindberg N, Chamlin SL, et al. | AI algorithm that accurately classifies infantile hemangiomas from clinical images |
| 11 | Assessing the performance of artificial intelligence models in evaluating inflammatory skin disease severity: a systematic review and meta-analysis | Cai ZR, Kim J, Rezaei SJ, et al. | AI models show strong performance in assessing severity of common inflammatory skin diseases and reliably distinguish them compared to dermatologist scoring systems |
| 12 | Early intervention and disease modification in atopic dermatitis-the current state of the field and barriers to progress | Jacobson ME, Seshadri RS, Morimoto R, et al. | Early diagnosis and intervention in pediatric atopic dermatitis can improve long-term outcomes |
| 13 | Enhanced early skin treatment for atopic dermatitis in infants reduces food allergy | Yamamoto-Hanada K, Kobayashi T, Mikami M, et al. | Early skin treatment for infant atopic dermatitis significantly reduced the incidence of hen’s egg allergy compared with conventional reactive treatment |
| 14 | Disparities in dermatology AI performance on a diverse, curated clinical image set | Daneshjou R, Vodrahalli K, Novoa RA, et al. | AI models showed decreased performance on diverse image datasets for darker skin tones and rare conditions |
| 15 | Disparities in Health Care and the Digital Divide | Saeed SA, Masters RM. | Digital access gaps contribute to persistent health care disparities, limiting the reach and benefits for underserved populations |
| 16 | Stigmatization and Mental Health Impact of Chronic Pediatric Skin Disorders | Paller AS, Rangel SM, Chamlin SL, et al. | Chronic pediatric skin disorders are strongly associated with stigma, which correlates with reduced quality of life, increased anxiety and depression, and poorer peer relationships in affected children |
| 17 | Risk of Mental Disorders in Children and Adolescents With Atopic Dermatitis: A Systematic Review and Meta-Analysis | Xie QW, Dai X, Tang X, Chan CHY, Chan CLW. | Children and adolescents with atopic dermatitis have a significantly increased risk of developing mental health disorders |
| 18 | Ethical considerations for artificial intelligence in dermatology: a scoping review | Gordon ER, Trager MH, Kontos D, et al. | Identifies key ethical principles for AI in dermatology such as fairness, inclusivity, and transparency |
| 19 | Lack of Transparency and Potential Bias in Artificial Intelligence Data Sets and Algorithms: A Scoping Review | Daneshjou R, Smith MP, Sun MD, Rotemberg V, Zou J. | Highlights the lack of transparency and potential for bias in AI datasets and algorithms |
| 20 | Challenges of artificial intelligence in medicine and dermatology | Grzybowski A, Jin K, Wu H. | Identifies key challenges for AI in medicine and dermatology including bias, lack of transparency, ethical concerns, data security, and unequal access |
AI diagnostic applications
Artificial intelligence (AI) describes a system of computers that uses innovative algorithms and computational models to simulate aspects of human thinking and analysis. With recent advancements in big data, processing power, and algorithm development, AI is being increasingly integrated into everyday life, with promising abilities in healthcare. From identifying at-risk patients to preventive care screenings, AI has the potential to expand clinicians’ reach while improving efficiency. Healthcare providers must balance the application of AI to ensure it complements, rather than replaces, the human touch in patient care.6
AI has the potential to both alleviate and exacerbate health inequities. This is impacted by factors including access, trust, dehumanization, autonomy, bias, and community effects, as summarized in Table 2.
These factors are especially relevant for rural and underserved communities, which are already disproportionately affected by limited access to specialists. When this is taken into consideration, AI can extend dermatologic expertise into settings where pediatric dermatologists are scarce.7
Several studies illustrate the promise of AI in pediatric dermatology. A 2021 randomized clinical trial investigated how AI tools can help primary care providers accurately diagnose skin conditions. The AI model used a convolutional neural network to assess over 16,000 images across almost 420 skin conditions, with diagnoses confirmed by board-certified dermatologists. In this study, 40 primary care providers, including 20 physicians and 20 nurse practitioners, submitted images of skin disorders found in the clinic to the tool and then received differential diagnoses. AI-aided clinical assessments agreed with a dermatologist’s assessment, with an improvement of 47% to 58% (p<0.001). This was found to be equivalent to 1 additional correct diagnosis per 8 to 10 cases.8 Such tools can help providers triage pediatric skin conditions more effectively by prioritizing urgent referrals and reducing delays in care, especially for malignant or rapidly proliferating lesions. Infantile hemangiomas, for example, are one of the most common pediatric tumors and have the potential to cause permanent disfigurement and comorbid conditions due to their rapid growth.9 To address this concern, a similar algorithm was trained with over 5,800 images of facial infantile hemangiomas diagnosed by a dermatologist. The algorithm achieved 91.7% accuracy in diagnosing the lesion, with a sensitivity of 93%.10 Identifying such lesions correctly is vital for timely intervention, especially in vulnerable regions like the face.
AI for severity assessment
A meta-analysis evaluated the performance of AI tools in assessing the severity of common skin conditions, such as acne, eczema, and warts. The results showed strong diagnostic performance, with AI models achieving a pooled sensitivity of 80.5% and reliably distinguishing moderate-to-severe disease from dermatologist scoring systems such as the Eczema Area and Severity Index (97.3%), Investigator’s Global Assessment (78.9%), or Hayashi grading (89.7%).11 For children in underserved areas, this sensitivity ensures that significant disease is not overlooked. Early identification through AI-assisted screening could allow prompt initiation of therapies such as topical corticosteroids for atopic dermatitis, which are known to reduce allergic sensitization and improve quality of life.12 For example, treatment with topical corticosteroids for secondary prevention decreased the risk of developing an allergy to chicken egg compared with conventional therapy (31.4% vs 41.9%, p = 0.0028).13 Thus, earlier identification of skin disease with AI tools can not only alleviate symptoms but also decrease the risk of other potential health conditions.
Social determinants and equity considerations
The use of AI in pediatric dermatology can only be integrated into healthcare effectively if it is designed with accessible and inclusive datasets. Rural and underserved communities are particularly vulnerable to inequities if algorithms are not created with inclusivity in mind. These datasets must include information on the social determinants of health, such as race, geographic location, socioeconomic status, and digital access. A 2022 study highlighted this risk using the Diverse Dermatology Images dataset, which includes a broad spectrum of skin tones and uncommon biopsy-confirmed dermatologic conditions. Compared to standard datasets, AI performance in correctly distinguishing between correct and incorrect diagnoses decreased by 27-36%, with the most significant declines observed in darker skin tones and presentations of rare diseases. Without deliberate inclusion of such populations, AI risks perpetuating existing disparities rather than reducing them.14
Barriers to accessibility also extend to technology itself. For AI to best be utilized in healthcare, there must be digital literacy, reliable internet service, and readily available devices within the community. Without these factors, the use of AI is severely limited. If left unaddressed, these challenges risk excluding the very populations most in need of care, particularly those living in rural communities where access to technology may be scarce. To prevent this, infrastructure changes are necessary to fund technological services and provide community education on these technologies.15
Psychosocial implications
Chronic skin disorders often begin in childhood and influence both physical health and psychological and social well-being. Stigmatization, or the association of discriminatory and false views with a person, can have profound effects on children with visible skin disease, whether self-perceived or imposed by others. In a cohort of 1671 children aged 8-17 with chronic skin conditions, 56.4% reported high visibility of disease, and 43.8% reported at least moderate stigma. Acne, atopic dermatitis, and vitiligo were among the most visible conditions. Stigma was strongly associated with a reduction in quality of life, an increase in depression and anxiety (p<0.001), and poor peer relationships.16 Furthermore, a related study found that children with atopic dermatitis had 65.2% increased odds of developing a mental health disorder when compared to peers without the skin condition. Specifically, children with atopic dermatitis had a significantly higher risk of comorbid conditions of ADHD, sleep disorders, and depression (p<0.001). Race further contributed to these odds, with minority children experiencing even greater risk. These findings highlight the psychosocial burden of pediatric skin conditions and emphasize the importance of early detection and intervention.17
AI has the potential to reduce the visibility and severity of disease by assisting providers in early identification of skin disorders, enabling more efficient management. By treating the disease at the beginning of the clinical course, it can reduce the risk of psychosocial distress that the disease would have caused. In addition, patients and families can be connected earlier with appropriate mental health support and resources, integrating dermatologic care with broader child well-being.
Challenges and ethical considerations
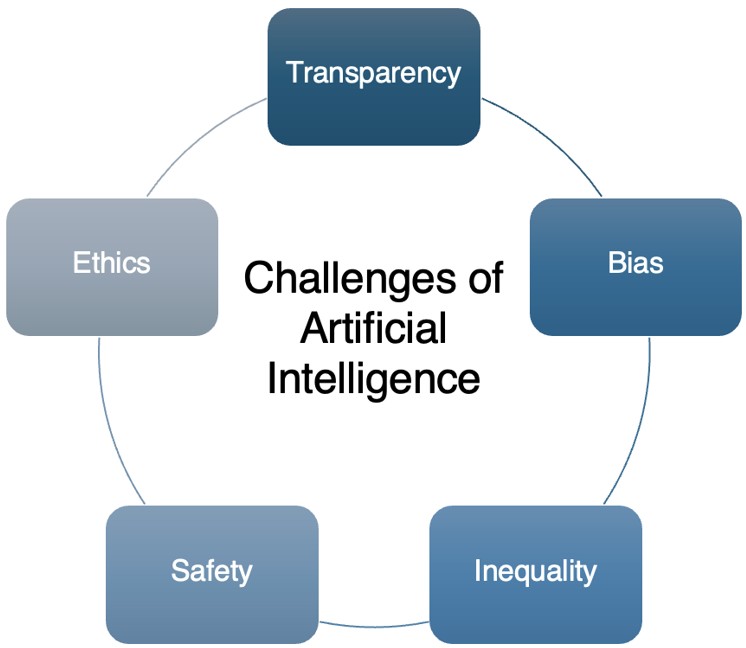
While AI holds promise in pediatric dermatology, its integration raises challenges for ensuring safety and equity in clinical practice. Algorithmic bias remains a significant concern given that children of color are underrepresented in training datasets.18 A recent review of dermatologic AI studies found that 20% indicated data on race or ethnicity, and only 10% included information on skin tone, indicating a lack of transparency within data.19 Other challenges include privacy concerns, informed consent, and the protection of minors, given the reliance on sensitive image and health data. For example, many AI algorithms have limited explainability in how the tool reached a clinical diagnosis, which may impede shared decision-making and concerns of consent for not only minors, but all patients.20 These challenges are summarized in Figure 2, created by the authors for this review.
Underserved communities may face additional barriers, such as poor internet access and low image quality, which further limit their effectiveness. When implementing new technologies, providers should work with patients to understand their level of understanding of technology. Educating patients on how to tailor the use of AI to their needs correctly is the first step towards reducing the challenges faced in these communities. Building trust with communities and designing diverse algorithms are vital steps to ensure AI is improving care rather than deepening disparities.20
DISCUSSION
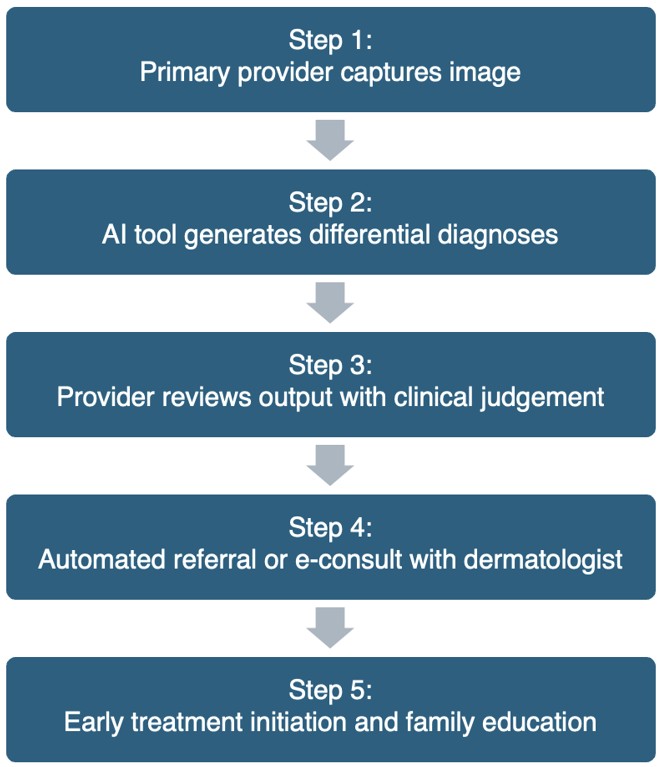
This review demonstrates that AI has the potential to close gaps in pediatric dermatologic care by increasing access to specialist-level support in rural and underserved communities. Across the literature, AI technologies show promising diagnostic performance, with broader significance in their ability to reduce triage delays, enabling prompt therapeutic interventions. Current evidence suggests that AI functions best when complementing clinician judgement, rather than replacing it. Integrating AI into pediatric workflows may help primary care providers triage more effectively, reduce unnecessary referrals, and initiate appropriate management earlier. This is particularly impactful for addressing children’s disease course, quality of life, and psychosocial outcomes. A proposed model for AI integration for pediatric skin conditions is summarized in Figure 3, created by the authors for this review.
This review has several limitations that should be considered when interpreting its findings. Current existing literature reviews mainly focus on adult dermatology or the general use of AI. In comparison, this review investigates disparities that are specific to the pediatric population, as children have specific disease patterns, developmental milestones, and psychosocial considerations that are often underrepresented in AI training datasets. The few studies that validate the use of AI tools in pediatric or rural clinics limit their generalizability and raise questions about the equitable implementation of AI. Another limitation is that this review includes only studies in English and may be geographically biased toward the United States, which may hinder understanding of AI use in underserved regions. The narrative nature of this review also introduces the possibility of selection bias, as a formal meta-analysis was not feasible given the study designs and outcomes. Furthermore, as AI technologies continue to evolve, newer models or studies may have emerged since the time of the literature collection.
Thus, clinicians should consider using AI to aid diagnosis and disease management, and policymakers should prioritize funding equitable AI technologies. Future research should focus on creating diverse training datasets to minimize bias, strengthening the integration of AI into electronic health records, and developing technological infrastructure in rural and underserved communities. Longitudinal studies that investigate clinical adherence, health outcomes, and patient satisfaction can provide essential information to guide responsible, equitable adoption of AI in pediatric dermatology.
CONCLUSION
Artificial intelligence offers a unique opportunity to improve the quality of pediatric dermatologic care, particularly for children in rural and underserved communities. By extending specialist support into primary care, AI has the potential to improve access, accuracy, and timeliness of patient care. Attaining these benefits will require a continued commitment to the development of equitable models, careful clinical integration, and ongoing evaluation. With appropriate safeguards, AI can strengthen pediatric dermatologic care and help ensure that all children receive timely, high-quality care regardless of geographic or socioeconomic barriers.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Prindaville B, Antaya RJ, Siegfried EC. Pediatric dermatology: past, present, and future. Pediatr Dermatol. 2015;32:1-12. https://doi.org/10.1111/pde.12362
- Sinha S, Lin G, Zubkov M, Wu R, Feng H. Geographic distribution and characteristics of the pediatric dermatology workforce in the United States. Pediatr Dermatol. 2021;38:1523-8. https://doi.org/10.1111/pde.14824
- Chaudhry SB, Armbrecht ES, Shin Y, et al. Pediatric access to dermatologists: medicaid versus private insurance. J Am Acad Dermatol. 2013;68:738-48. https://doi.org/10.1016/j.jaad.2012.10.034
- Prindaville B, Horii KA, Siegfried EC, Brandling-Bennett H. Pediatric dermatology workforce in the United States. Pediatr Dermatol. 2019;36:166-8. https://doi.org/10.1111/pde.13684
- Desrosiers AS, Ibrahim JM, Jacks SK. A barrier to care: distance traveled affects adherence to treatment and follow-up plans for patients with infantile hemangioma. Pediatr Dermatol. 2019;36:402-3. https://doi.org/10.1111/pde.13788
- Chen M, Decary M. Artificial intelligence in healthcare: an essential guide for health leaders. Healthc Manage Forum. 2020;33:10-8. https://doi.org/10.1177/0840470419873123
- d’Elia A, Gabbay M, Rodgers S, et al. Artificial intelligence and health inequities in primary care: a systematic scoping review and framework. Fam Med Community Health. 2022;10:e001670. https://doi.org/10.1136/fmch-2022-001670
- Jain A, Way D, Gupta V, et al. Development and assessment of an artificial intelligence-based tool for skin condition diagnosis by primary care physicians and nurse practitioners in teledermatology practices. JAMA Netw Open. 2021;4:e217249. https://doi.org/10.1001/jamanetworkopen.2021.7249
- Rodríguez Bandera AI, Sebaratnam DF, Wargon O, Wong LCF. Infantile hemangioma. Part 1: epidemiology, pathogenesis, clinical presentation and assessment. J Am Acad Dermatol. 2021;85:1379-92. https://doi.org/10.1016/j.jaad.2021.08.019
- Zhang AJ, Lindberg N, Chamlin SL, et al. Development of an artificial intelligence algorithm for the diagnosis of infantile hemangiomas. Pediatr Dermatol. 2022;39:934-6. https://doi.org/10.1111/pde.15149
- Cai ZR, Kim J, Rezaei SJ, et al. Assessing the performance of artificial intelligence models in evaluating inflammatory skin disease severity: a systematic review and meta-analysis. Br J Dermatol. 2025;193:847-55. https://doi.org/10.1093/bjd/ljaf250
- Jacobson ME, Seshadri RS, Morimoto R, et al. Early intervention and disease modification in atopic dermatitis-the current state of the field and barriers to progress. J Eur Acad Dermatol Venereol. 2024;38:665-72. https://doi.org/10.1111/jdv.19699
- Yamamoto-Hanada K, Kobayashi T, Mikami M, et al. Enhanced early skin treatment for atopic dermatitis in infants reduces food allergy. J Allergy Clin Immunol. 2023;152:126-35. https://doi.org/10.1016/j.jaci.2023.03.008
- Daneshjou R, Vodrahalli K, Novoa RA, et al. Disparities in dermatology AI performance on a diverse, curated clinical image set. Sci Adv. 2022;8:eabq6147. https://doi.org/10.1126/sciadv.abq6147
- Saeed SA, Masters RM. Disparities in health care and the digital divide. Curr Psychiatry Rep. 2021;23:61. https://doi.org/10.1007/s11920-021-01274-4
- Paller AS, Rangel SM, Chamlin SL, et al. Stigmatization and mental health impact of chronic pediatric skin disorders. JAMA Dermatol. 2024;160:621-30. https://doi.org/10.1001/jamadermatol.2024.0594
- Xie QW, Dai X, Tang X, Chan CHY, Chan CLW. Risk of mental disorders in children and adolescents with atopic dermatitis: a systematic review and meta-analysis. Front Psychol. 2019;10:1773. https://doi.org/10.3389/fpsyg.2019.01773
- Gordon ER, Trager MH, Kontos D, et al. Ethical considerations for artificial intelligence in dermatology: a scoping review. Br J Dermatol. 2024;190:789-97. https://doi.org/10.1093/bjd/ljae040
- Daneshjou R, Smith MP, Sun MD, Rotemberg V, Zou J. Lack of transparency and potential bias in artificial intelligence data sets and algorithms: a scoping review. JAMA Dermatol. 2021;157:1362-9. https://doi.org/10.1001/jamadermatol.2021.3129
- Grzybowski A, Jin K, Wu H. Challenges of artificial intelligence in medicine and dermatology. Clin Dermatol. 2024;42:210-5. https://doi.org/10.1016/j.clindermatol.2023.12.013
Copyright and license
Copyright © 2026 The author(s). This is an open-access article published by Aydın Pediatric Society under the terms of the Creative Commons Attribution License (CC BY) which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.