Abstract
Objective: This study aimed to evaluate the effect of training teachers using the video simulation method on their knowledge of epileptic seizure management and on their first-aid intervention skills.
Methods: A survey was distributed to 250 participating teachers working in both private and public schools. The survey included basic demographic information, teachers’ awareness of epilepsy, and their knowledge of first aid measures. Subsequently, the teachers received a training session on general information about epilepsy, first response to epileptic seizures, and emergency procedures using the video simulation training method. Awareness and attitudes were reassessed using the same survey.
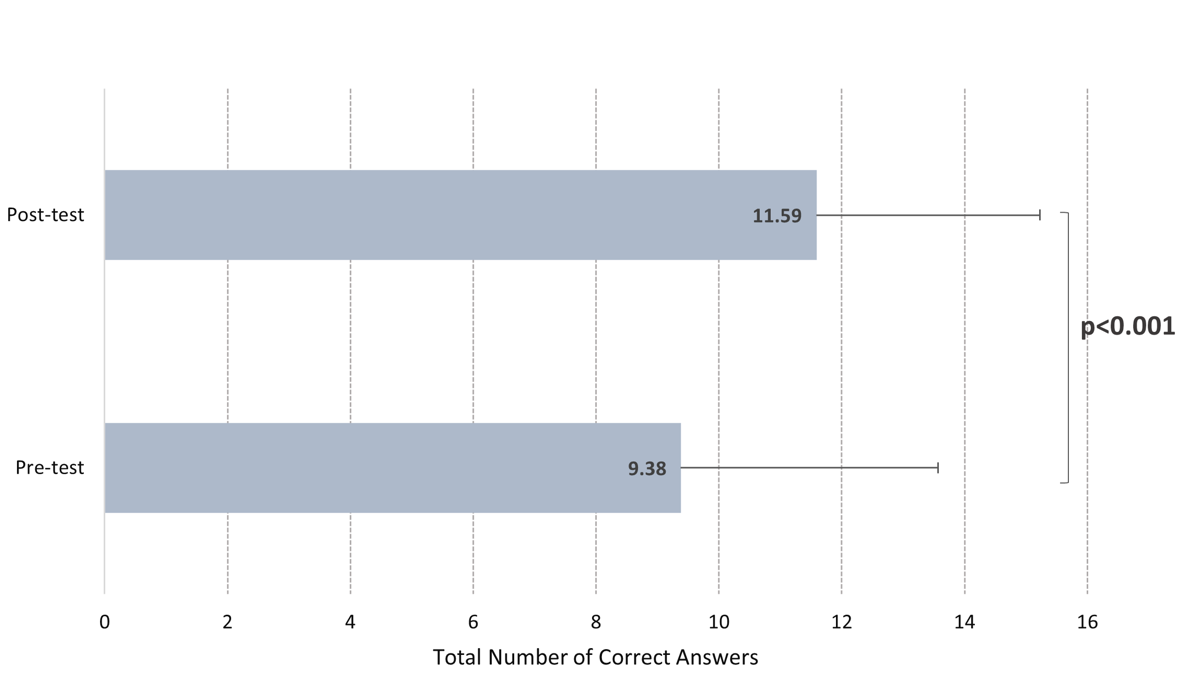
Results: The study involved 250 participants with an average age of 39.76 years, 62.8% female, and 78.4% working in the public sector. Participants with connections to individuals with epilepsy had significantly higher pre-training correct response scores (p=0.026, p=0.001). 72.8% had received first-aid training, and 26.6% had performed first aid, but only 6.1% considered their knowledge sufficient. Before training, 94.4% recognized epilepsy as a neurological disorder. The awareness of epilepsy being treatable increased from 70.7% to 90.4% (p<0.001). Knowledge of proper seizure interventions significantly improved, with correct responses to questions about safe positioning and jaw clenching rising from 52.4% to 78.4% and 52.4% to 90.8%, respectively (p<0.001). The total number of correct answers significantly increased after training, from 9.38 ± 4.18 to 11.59 ± 3.64 (p<0.001).
Conclusion: These findings indicate that video simulation training is an effective method for improving teachers’ knowledge and first-aid skills in managing epileptic seizures, supporting the integration of structured simulation-based interventions into school-based emergency preparedness programs.
Keywords: epilepsy, first-aid management, school teachers, educational video
INTRODUCTION
Epilepsy is a common chronic neurological disorder and a significant public health issue.1 Globally, 4–10% of children experience at least one seizure by age 16, with about one-third occurring in schools.1,2 This highlights the critical role of teachers as first responders, responsible for ensuring the child’s safety and providing seizure first aid.
Epilepsy is considered a neurological emergency due to the sudden and unpredictable onset of seizures, which can be life-threatening if not promptly and correctly managed. Seizures may be distressing for both the patient and observers, and inadequate first aid can lead to injury or death.3 Special attention is needed in school and work settings, where trained individuals can ensure safety during seizures, provide appropriate post-seizure care, and seek medical assistance when necessary. Public education and awareness programs can promote safer social participation for individuals with epilepsy and help reduce disease-related stigma.3,4 Children with epilepsy may face additional challenges at school, including social isolation, learning difficulties, and stigmatization.5
Teachers’ knowledge of epilepsy and seizure first aid is crucial for student safety and well-being.5 Studies indicate that teachers’ misconceptions about epilepsy negatively impact the educational experiences of children with the condition.3,6 Teachers’ knowledge and attitudes can directly influence students’ academic performance, development, and self-confidence. During a seizure, teachers are responsible for preventing injury, providing appropriate post-seizure care, and seeking medical assistance when necessary, as improper interventions may cause secondary harm.7 Seizures lasting longer than five minutes or occurring consecutively indicate status epilepticus, which requires immediate medical attention. Early recognition and referral are crucial to prevent serious neurological and systemic complications.8
To enhance teachers’ knowledge and preparedness in managing epileptic seizures, video simulation training offers an innovative instructional approach that combines visual demonstration with scenario-based learning. Video simulation training is widely used in clinical and emergency education to support both knowledge acquisition and practical skill development.9 This approach incorporates elements such as interactive video content, branching scenarios, role-model demonstrations, and expert commentary, aiming to help learners develop both cognitive and affective skills within a safe and controlled setting.9 Video simulation training is a hybrid model that fits naturally with existing training approaches.10 In this study, a video simulation was created based on current evidence on epileptic seizure management.
The aim of this study was to innovatively enhance teachers’ competencies in providing accurate first aid to students experiencing seizures and to investigate changes in their knowledge and attitudes toward seizure management before and after a video simulation–based training program specifically designed for effective seizure management in the school setting.
MATERIALS AND METHODS
Study design
This cross-sectional study was conducted between November 15 and December 31, 2022. Following approval from the ethics committee and obtaining the necessary permissions from the Ministry of National Education, 250 teachers working in private and public schools affiliated with the Provincial Directorate of National Education were included in the study. Data were collected using survey forms administered before and after a three-minute clinical simulation training video titled “First Approach to a Child Having a Seizure.”
Sample size and sampling procedure
The target population and sample size were determined based on previous studies.11 Using OpenEpi, the minimum sample size required to detect at least a 20% change between pre-test and post-test responses was calculated as 118, with 95% confidence and 90% power.12 Due to higher-than-expected voluntary participation, all eligible teachers who consented were included, resulting in a final sample of 250 participants, which enhanced the study’s statistical power.
Data collection tools
The data collection instrument was adapted from a prior study, with context-appropriate modifications to ensure its suitability for the current research objectives.13 These modifications included adjustments to item wording, alignment with the target population, and refinement of response options for improved clarity. Following the adaptation process, the instrument was reviewed for content relevance and comprehensibility. It was then administered to volunteer teachers from the designated schools, selected according to predetermined inclusion criteria, to obtain the data necessary for the study.
In the video simulation, seizure management was explained step by step and demonstrated on a mannequin experiencing a seizure, in accordance with evidence from the literature. The questionnaire was first administered to participants before the training video. Following this pre-test, the teachers watched the video simulation training video (Appendix 1). After viewing the video, the same questionnaire, consisting of identical items, was re-administered as a post-test to assess changes in knowledge. The first section of the 25-item questionnaire assessed participants’ sociodemographic characteristics, including age, gender, length of professional experience, family history of epilepsy, prior knowledge about epilepsy, and first-aid knowledge. The second section evaluated teachers’ knowledge of epilepsy and appropriate interventions during an epileptic seizure. For knowledge assessment, each correct response was scored as “1” and each incorrect response as “0”; unanswered items were excluded from scoring. The total score for all knowledge items was 21. To evaluate the effect of the training, the difference between pre-test and post-test correct response rates was analyzed, reflecting improvements in participants’ knowledge and their ability to provide correct interventions during seizures.
Video simulation training
The video aimed to provide a standardized, structured, and reproducible educational experience for all participants. The educational content and seizure management steps in the video were aligned with current recommendations from the International League Against Epilepsy (ILAE) and internationally accepted first-aid principles for seizure management (https://www.cdc.gov/epilepsy/first-aid-for-seizures/index.html).14 The video was simulated by a pediatric neurologist and clinical educators experienced in pediatric emergency care and simulation-based education. Prior to implementation, the video content was reviewed by two pediatric neurology experts and one simulation-based education specialist. They evaluated the scenario, seizure description, demonstrated interventions, and pedagogical coherence. Minor revisions were made based on their feedback to ensure adherence to best practices. The video clearly defined learning objectives, aiming to improve teachers’ knowledge, first-aid skills, and appropriate decision-making during seizure events in the school setting.
Video content summary
In this study, the video simulation was developed based on current literature on seizure management and included both theoretical and practical components (Appendix 2). In the first 1 minute and 10 seconds, the video provided brief information on epilepsy, seizure types, treatment principles, and the importance of correct first aid. From 1:10 to 2:52, a child seizure scenario was narrated: a previously healthy boy suddenly collapses while playing, exhibiting limb stiffness, shaking, upward eye deviation, and jaw clenching. During this segment, seizure management steps were demonstrated on a manikin, highlighting correct interventions while verbally emphasizing actions to avoid. In the final segment (2:52–3:02), conditions requiring activation of emergency medical services were displayed on the screen and read aloud. This video provided a standardized, structured, and reproducible educational experience for all participants. The simulation used in this study is provided in Appendix 2.
Statistical analysis
Normality assumptions were examined with kurtosis and skewness values. If the kurtosis and skewness coefficients were within ±2, it was accepted that the data were in compliance with a normal distribution.15 We used an independent two-sample t-test to compare the pre-test and post-test total correct answers between two groups, assuming a normal distribution. One-way analysis of variance (ANOVA) was used to compare pre- and post-test total correct answers, assuming a normal distribution across three or more groups. Variance homogeneity was examined using the Levene test, and the F test was evaluated when homogeneity was achieved. In cases of significant difference in ANOVA results, multiple comparisons were examined using the Duncan test under the assumption of homogeneity of variances. A paired two-sample t-test was used to compare the total correct numbers of pre-test and post-test with a normal distribution. Comparisons between pre-test and post-test in categorical data were examined using McNemar’s test for two-time two-category data and the Stuart-Maxwell (Marginal Homogeneity) test for two-time three-category data. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 26.0 (IBM Corp., Armonk, NY, USA), and a p-value of <0.05 was considered statistically significant.
RESULTS
The study included 250 participants with a mean age of 39.76 years (range: 25–65). Of the participants, 62.8% were female, and 78.4% were employed in public schools. Regarding the educational level at which they taught, 44.8% worked in elementary schools, while 33.2% were primary school teachers. Descriptive statistics on the participants’ demographic characteristics are presented in Table 1.
| SD: Standard Deviation, min: minimum, max: maximum. | ||
| Table 1. Descriptive statistics of the participants’ demographic characteristics | ||
| Characteristics |
|
|
| Age |
|
|
| Sex | ||
| Female |
|
|
| Male |
|
|
| School type | ||
| Public |
|
|
| Private |
|
|
| School education level | ||
| Daycare/Preschool |
|
|
| Primary School |
|
|
| Middle School |
|
|
| High School |
|
|
| Teaching field | ||
| Primary school teacher /Elementary school teacher |
|
|
| Special education teacher |
|
|
| Mathematics teacher |
|
|
| English language teacher |
|
|
| School counselor /Guidance and psychological counselor |
|
|
| Early childhood education teacher |
|
|
| Turkish language teacher |
|
|
| Religious culture and ethics teacher |
|
|
| Social studies teacher |
|
|
| Science teacher / general science teacher |
|
|
| Physical education teacher |
|
|
| Music teacher |
|
|
| Biology teacher |
|
|
| Chemistry teacher |
|
|
| Visual arts teacher |
|
|
| Technology and design teacher |
|
|
| Physics teacher |
|
|
| Geography teacher |
|
|
| Computer science teacher / Ict teacher |
|
|
| German/Arabic language teacher |
|
|
| Health sciences teacher |
|
|
| Years of teaching experience | ||
| 1-5 |
|
|
| 6-10 |
|
|
| > 10 |
|
|
| Do you have epilepsy? | ||
| Yes |
|
|
| No |
|
|
| Do you know anyone with epilepsy? | ||
| Yes |
|
|
| No |
|
|
| Do you have students with epilepsy? | ||
| Yes |
|
|
| No |
|
|
| Have you ever received first aid training? | ||
| Yes |
|
|
| No |
|
|
| Sufficient first aid knowledge? | ||
| Yes |
|
|
| No |
|
|
| Partially |
|
|
In the study, 0.8% of the participants reported having epilepsy, while 11.6% indicated that they had close relatives with the condition. Additionally, 30.4% stated that they had at least one student with epilepsy in their schools. Participants who had relatives or students with epilepsy demonstrated significantly higher mean pre-training correct response scores compared with those who did not (p = 0.026 and p = 0.001, respectively).
Among the participants, 26.6% (n= 66) reported having previously administered first aid. In response to the question, “Do you think your first-aid knowledge is sufficient?”, 6.1% (n= 15) answered “Yes,” 60.2% (n=147) answered “No,” and 33.6% (n= 82) responded “Partially.” Additionally, 72.8% (n=182) had received prior first-aid training, with most participants reporting having obtained it from various sources. Among those who had received first-aid training, 61.2% (n=153) had attended face-to-face courses or training, 9.6% (n=24) had self-taught using informal online resources (such as informational websites or videos), and 7.2% (n=18) had completed structured online courses or formal training programs.
According to the participants, 59.3% (n=147) had previously witnessed someone experiencing an epileptic seizure. When examining their reactions to witnessing an epileptic seizure, the following responses were noted: 11.6% reported feeling “fear,” 12.4% “panic,” 2% “I distanced myself from the scene,” 6.8% “I did nothing,” and 2% selected “other”. On the other hand, in terms of positive responses, 33.2% stated that they “assisted,” and 16.8% reported that they “ immediately called the emergency medical services number (112).”
Analysis of participants’ knowledge revealed significant improvements following the training (Table 2). Recognition of epilepsy as a treatable condition increased markedly (70.7% to 90.4%, p <0.001). Awareness of key seizure characteristics—including behavioral arrest, involuntary facial movements, limb contractions, and incoherent speech—also improved significantly (p ≤ 0.002 for all). The proportion selecting “all of the above” rose from 15.6% to 28.0% (p = 0.001), while the percentage reporting no knowledge declined from 2.4% to 0% (p = 0.030). No significant changes were observed for generalized muscle contractions or memory impairment (p> 0.05). Overall, the training substantially enhanced teachers’ understanding of epilepsy and seizure presentation.
| mc: McNemar test, sm: Stuart–Maxwell test, n (%), p-value of <0.05. | |||||
| Table 2. Evaluation of participants' knowledge levels regarding epilepsy disease | |||||
| Related questions |
|
|
|
||
|
|
|
|
|
||
| Is epilepsy a treatable condition? | |||||
| Yes |
|
|
|
||
| No |
|
|
|||
| What kind of condition is epilepsy? | |||||
| Psychological |
|
|
|
||
| Supernatural |
|
|
|||
| Neurological |
|
|
|||
| I have no knowledge |
|
|
|||
| How would you describe an epileptic seizure? | |||||
| Staring at a single point and appearing lost in thought |
|
|
|
|
|
| Involuntary facial expressions and movements, such as lip biting |
|
|
|
|
|
| Generalized body stiffness and trembling |
|
|
|
|
|
| Stiffness and trembling in a single body part |
|
|
|
|
|
| Incoherent speech and repetitive movements |
|
|
|
|
|
| Memory loss to the extent of distraction |
|
|
|
|
|
| None of the above |
|
|
|
|
|
| All of the above |
|
|
|
|
|
| I don't know |
|
|
|
|
|
Significant improvements were observed in participants’ knowledge regarding safe positioning during an epileptic seizure (Table 3). The proportion selecting “move the person to a safe place” increased from 52.4% to 78.4% (p <0.001), and those choosing “turn the person onto their left side to facilitate breathing” rose from 45.6% to 84.4% (p <0.001). Similar significant gains were noted for “prevent vomit from entering the lungs” and “place a soft pillow under the head” (p <0.001). The percentage of participants reporting “I have no knowledge/no opinion” declined from 15.2% to 0% (p <0.001).
| mc: McNemar test, n (%), p-value of <0.05. | ||||||
| Table 3. Comparison of participants' knowledge levels on epileptic seizure management | ||||||
| Related questions |
|
|
|
|||
|
|
|
|
|
|||
| What actions should be taken to ensure a safe position for someone having an epileptic seizure? | ||||||
| The individual should be moved to a safe location |
|
|
|
|
|
|
| The person should be turned onto their left side to facilitate easier breathing |
|
|
|
|
|
|
| The individual should be turned onto their left side to prevent aspiration of stomach contents in case of vomiting |
|
|
|
|
|
|
| Clothing that may restrict breathing, such as ties, and breakable items like glasses should be removed |
|
|
|
|
|
|
| The person should be positioned with their head lower than their feet |
|
|
|
|
|
|
| A soft pillow should be placed under the individual's head |
|
|
|
|
|
|
| The person should be left in place without interference or intervention |
|
|
|
|
|
|
| I don't know / I have no opinion |
|
|
|
|
|
|
| What should be done if an individual having an epileptic seizure has a clenched jaw? | ||||||
| Attempt to open the mouth by inserting objects such as a fork or spoon |
|
|
|
|
|
|
| Attempt to open the mouth with fingers |
|
|
|
|
|
|
| Immediately call an ambulance |
|
|
|
|
|
|
| Ensure a safe position and wait for the seizure to stop |
|
|
|
|
|
|
| I don’t know / I have no opinion |
|
|
|
|
|
|
| Which of the following interventions are correct for an individual having an epileptic seizure? | ||||||
| The person is exposed to the smell of onion or garlic |
|
|
|
|
|
|
| The person is exposed to the smell of cologne |
|
|
|
|
|
|
| A slap is applied |
|
|
|
|
|
|
| The body is shaken |
|
|
|
|
|
|
| Sugar water is given to the person |
|
|
|
|
|
|
| Water is poured on the person |
|
|
|
|
|
|
| Cardiopulmonary resuscitation is performed |
|
|
|
|
|
|
| Artificial respiration is given |
|
|
|
|
|
|
| A safe position is ensured, and the seizure is allowed to stop |
|
|
|
|
|
|
| I don’t know / I have no opinion |
|
|
|
|
|
|
| When would you call an ambulance for an individual having an epileptic seizure? | ||||||
| Immediately |
|
|
|
|
|
|
| Never |
|
|
|
|
|
|
| If the seizure lasts longer than 5 minutes |
|
|
|
|
|
|
| If there is discoloration or blueness in the skin |
|
|
|
|
|
|
| If consciousness and respiration do not return to normal after the seizure |
|
|
|
|
|
|
| If the individual has another seizure without regaining consciousness after the first one |
|
|
|
|
|
|
| If confusion or disorientation persists an hour after the seizure |
|
|
|
|
|
|
| If a serious injury occurred during the seizure |
|
|
|
|
|
|
Following the training, participants’ knowledge regarding jaw clenching during an epileptic seizure improved significantly (Table 3). The proportion selecting unsafe interventions—such as inserting objects into the mouth or forcibly opening it—decreased (p <0.001), while those choosing “provide a safe position and allow the seizure to stop” increased from 52.4% to 90.8% (p <0.001). The percentage reporting “I have no knowledge/no opinion” declined from 14% to 0% (p <0.001), and the selection of “all of the above” also decreased significantly (p = 0.035).
The training led to significant improvements in participants’ knowledge of correct interventions (Table 3). Selections of ineffective measures, such as “smelling onion or garlic” and “smelling cologne,” decreased (p = 0.039 and p = 0.008), while choosing “provide a safe position and allow the seizure to stop” increased from 73.6% to 98% (p <0.001). The proportion reporting “I have no knowledge/no opinion” declined from 18% to 0.4% (p <0.001).
Participants’ knowledge regarding emergency response improved significantly after the training (Table 3). While nearly all participants correctly identified 112 as the emergency number both before and after the training, responses about when to call an ambulance during a seizure changed markedly. The proportion selecting “immediately” decreased (p <0.001), whereas selecting “if the seizure lasts longer than 5 minutes” increased from 0.8% to 84.4% (p <0.001). Significant increases were also observed for conditions such as cyanosis, failure of consciousness or breathing to return to normal, subsequent seizures without recovery, prolonged dizziness, and severe injury (p <0.001).
A significant increase was observed in the total number of correct answers after the training (pre-training: 9.38±4.18; post-training: 11.59±3.64; p < 0.001), indicating an overall improvement in participants’ knowledge (Figure 1). Before the training, significant differences in total correct answers were observed based on sex and institution type (Table 4). Females scored higher than males (p= 0.041), and public-school teachers outperformed those in private institutions (9.84 vs. 7.72, p = 0.001). Before the training, significant differences in total correct answers were observed based on school level, family history of epilepsy, and having students with epilepsy. Preschool/kindergarten teachers scored highest (12.41), while high school teachers scored lowest (8.69) (p= 0.015). Participants with relatives or students with epilepsy also scored higher than those without (11 vs. 9, p=0.026; 10.72 vs. 8.79, p=0.001). No significant difference was found based on years of professional experience (p=0.488).
| t: Independent samples t-test, f: One-way ANOVA, Test ist.: Test statistic, Mean± Standard deviation, a–b: Groups sharing the same letter do not differ significantly (Duncan test), p-value of <0.05. | ||||||
| Table 4. Comparison of pre- and post-test total correct scores according to demographic characteristics | ||||||
| Characteristics |
|
|
|
|
|
|
| Sex | ||||||
| Female |
|
|
|
|
|
|
| Male |
|
|
||||
| School Type | ||||||
| Public |
|
|
|
|
|
|
| Private |
|
|
||||
| School education level | ||||||
| Daycare/Preschool |
|
|
|
|
|
|
| Primary School |
|
|
||||
| Middle School |
|
|
||||
| High School |
|
|
||||
| Years of teaching experience | ||||||
| 1-5 |
|
|
|
|
|
|
| 6-10 |
|
|
||||
| > 10 |
|
|
||||
| Do you know anyone with epilepsy? | ||||||
| Yes |
|
|
|
|
|
|
| No |
|
|
||||
| Do you have students with epilepsy? | ||||||
| Yes |
|
|
|
|
|
|
| No |
|
|
||||
DISCUSSION
Epileptic seizures are acute clinical events that frequently require emergency intervention, and the implementation of correct first aid is essential to prevent injuries, reduce complications, and decrease mortality.16 The findings of this study demonstrate that video simulation training significantly improved teachers’ knowledge, attitudes, and intervention skills regarding epileptic seizures.
Teachers’ knowledge of epilepsy was found to be limited prior to the training program, with a mean total of correct answers of 9.38 ± 4.18, which increased to 11.59 ± 3.64 following the training. These findings align with previous studies indicating the presence of knowledge gaps regarding epilepsy among teachers.17 Consistent with previous national studies, our findings highlight that teachers’ first-aid knowledge and competence in managing seizures remain moderate despite prior training. For instance, a Turkish study involving 291 teachers reported that while those with first-aid training scored higher on self-efficacy scales, overall knowledge was still at a moderate level, with participants most frequently encountering minor injuries, bleeding, and seizures.18 Similarly, other studies in Turkey have demonstrated that teachers possess insufficient first-aid knowledge and exhibit limited awareness and practical skills in managing epilepsy and seizures.19,20 These consistent findings underscore the need for innovative and structured educational interventions, such as video simulation training, to effectively enhance teachers’ preparedness and confidence in responding to school-based emergencies.
When examining teachers’ total knowledge pre- and post-test scores, higher baseline levels were observed among female teachers, those working in public schools, preschool and primary school teachers, participants with students with epilepsy, and those with individuals with epilepsy in their immediate environment. Our findings are consistent with the existing literature and suggest that prior exposure to epilepsy—whether through professional experience or personal familiarity—together with demographic and institutional factors, may contribute to higher baseline knowledge.13,21,22 Pre-test scores differed across school levels, with preschool teachers demonstrating higher baseline knowledge, likely due to greater emphasis on child safety and first-aid training. Post-test scores showed no significant differences, indicating that video-simulation training effectively improved seizure first-aid knowledge across all groups, reducing initial disparities. These findings support the implementation of standardized training programs and align with previous studies showing higher first-aid knowledge among preschool and primary school teachers.19,23 On the contrary, a nationwide study conducted with 291 teachers from various educational levels across all provinces of Türkiye, using an online questionnaire, similarly reported that teachers’ first-aid knowledge levels were only moderate and that there were no significant differences between school levels.18 These findings suggest that deficiencies in first-aid knowledge are not limited to a particular educational stage but represent a systemic need across the entire school system.
Alkhotani et al. reported that private school teachers demonstrated higher pre-education awareness (81.3%) than public school teachers (49.8%), whereas post-education results showed a reversal, with public school teachers (88.5%) outperforming private school teachers (62.5%).24 This pattern suggests that education yields stronger gains among groups with lower baseline levels. In our study, public school teachers had significantly higher pre-test scores than private school teachers, whereas no significant difference remained in post-test scores. These findings collectively indicate that education reduces initial disparities between school types and contributes to leveling teachers’ knowledge.
Although this study aimed to assess seizure first aid knowledge among teachers of both sexes, the majority of participants (62.8%) were female, consistent with previous literature reporting higher participation of female teachers in education- and health-related studies.7,25 This greater interest among female teachers may reflect a higher awareness of the field. Another notable finding is that 33% of participants were primary school teachers. Given that this group is more likely to encounter neurological conditions such as epilepsy, it highlights the need for targeted seizure first-aid training for classroom teachers. Furthermore, guidance and special education teachers comprised 10.8% of the sample, indicating that this group frequently works with students with learning disabilities or special needs and is therefore more likely to encounter seizures, underscoring the importance of providing them with appropriate first-aid training.
The study findings indicate that 94.4% of teachers recognized epilepsy as a neurological disorder; however, their overall knowledge of first aid, seizure types, seizure management, and related topics was insufficient. This suggests that while basic awareness of epilepsy exists, more in-depth education is needed to develop a comprehensive understanding and enhance teachers’ practical skills. In a comparable study, 87.5% of teachers identified epilepsy as a neurological disorder, and 65.5% believed it to be treatable. Nevertheless, only 9.2% had received first-aid training, 52% reported that they would ensure safety and call for help during a seizure, and 64.8% indicated that they would position the student on their side and seek assistance after the seizure.26 In our study, although over half of the participants had received first-aid training, 63.8% had completed it more than five years ago. Nearly half of the participants correctly answered questions on seizure response. Additionally, 59.3% had previously witnessed a seizure, with 33.2% assisting and 16.8% immediately calling emergency services, while 11.6% reported fear, 12.4% panic, and 6.8% inaction. These findings indicate that although many participants were willing to intervene, anxiety and insufficient knowledge contributed to passive or avoidant behaviors. Similarly, Al Muslim et al. conducted a study with 423 teachers and found that 61.5% of them had insufficient knowledge about epilepsy. However, nearly half of the participants answered questions about how to respond during a seizure correctly.26 Many studies clearly indicate that there is a lack of sufficiently trained educators who have received first-aid training.7,27,28 This may reflect reliance on online research or past experiences, highlighting the need to use reliable guidelines and sources for accurate information.
Before the training, most teachers demonstrated limited knowledge of epilepsy, with 70.7% recognizing it as a treatable condition and 78% identifying seizures primarily as generalized convulsions, consistent with previous literature.24 Before the training, less common seizure manifestations—such as blankly at a fixed point, involuntary movements, lip biting, localized muscle contractions, incoherent speech, repetitive behaviors, and memory loss—were infrequently recognized. After the training, recognition of these symptoms significantly improved, highlighting the need for teachers to acquire comprehensive knowledge of different seizure types, including absence epilepsy, the most common form in children aged 6–11, accounting for approximately 18% of cases.29 Teachers are crucial in recognizing absence seizures. Initially, only 29.7% identified a blank stare as a symptom; this increased to 47.6% after training. Nonetheless, most teachers still failed to associate blank stares with seizures, highlighting the need for further training on subtle seizure types.
Video simulation-based first-aid training significantly improved teachers’ awareness and attitudes toward epilepsy. The proportion of participants correctly selecting “ensure a safe position and wait for the seizure to stop” when the jaw was clenched increased from 52.4% pre-training to 90.8% post-training. Similarly, correct responses regarding interventions to maintain a safe position increased significantly, indicating the training effectively enhanced knowledge and attitudes toward seizure management. İsler et al. reported that, before a modular training program, only 30% of healthcare professionals correctly identified the appropriate initial interventions for a child experiencing a seizure. After the training, this proportion increased to 70%, demonstrating the effectiveness of the program in improving seizure management skills among pediatric healthcare providers.11
Incorrect or delayed interventions during seizure first aid can lead to secondary injuries and serious complications, including status epilepticus.30 A study in Cameroon found that despite high knowledge, medical students still exhibited inappropriate attitudes and practices toward epileptic seizures.31 A systematic review revealed teachers’ insufficient knowledge and negative attitudes toward epilepsy, including limited awareness of its emergency management.24 This suggests that traditional beliefs and values established in society shape the perception of epilepsy. First-aid training and awareness campaigns based on accurate information can improve teachers’ competence, positively impact attitudes, and enhance the safety and quality of life for individuals with epilepsy. Using diverse materials—such as video simulations, brochures, case examples, and online content—can further engage teachers and improve knowledge retention. Tavares et al. evaluated the impact of a low-cost program comprising a brief educational video and booklet on teachers’ knowledge of epilepsy and seizure first aid.32 This aligns with our findings, showing a significant increase in teachers’ knowledge after training. The study also noted that the booklet alone had little impact, with the primary effect attributed to the video-based training.32 These results indicate that brief video trainings effectively enhance epilepsy awareness and should be more widely incorporated into educational programs, as supported by evidence on the benefits of multimedia-based learning.33 In our study, video simulation training presented practically on a model by a health professional was supported by visual and auditory components. It is reported in the literature that similar educational videos have a high impact on learning.11,33,34
In comparison with many studies conducted in Türkiye, the present study offers a broader scope and more robust methodology. Most national studies have focused exclusively on teachers working in preschool or primary education and have relied primarily on survey-based assessments, many of which demonstrated that teachers’ first-aid knowledge levels were below the desired competency.20,35 In contrast, our study includes teachers from all educational stages and employs both a structured questionnaire and a video-simulation–based training intervention. Therefore, it not only assesses baseline knowledge but also evaluates the effectiveness of an educational intervention, providing a methodological contribution to the national literature and offering a more comprehensive understanding of teachers’ seizure first-aid preparedness.
Methodological issues and limitations
This study has several methodological limitations. First, although the questionnaire was adapted from a previous study and reviewed by experts, formal construct validation and pilot testing were not conducted, and internal consistency (Cronbach’s α) could not be calculated due to the heterogeneous item structure. Second, the post-video questionnaire was administered again after a short interval, which may have limited the assessment of longer-term learning effects. Third, reliance on structured questionnaires may not fully capture the complexity of knowledge related to seizure management. Finally, the intervention relied solely on a video-based format; incorporating additional educational materials could have provided more comprehensive learning outcomes. These limitations should be considered when interpreting the findings.
CONCLUSION
This study aimed to evaluate the awareness of epilepsy and first aid among teachers through video simulation training. After the training, a significant increase was observed in teachers’ theoretical knowledge regarding intervention during seizures. The study results show that teachers improved their knowledge across all knowledge categories. This development provided by the training shows that teachers will be able to intervene in seizure cases more consciously and effectively in the future.
Ethical approval
This study has been approved by the Local Ethics Committee of Faculty of Medicine, Karadeniz Technical University (approval date 30.12.2001, number2021/319). Written informed consent was obtained from the participants.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Renzetti T, Calabrese C, Pietrafusa N, et al. Management of epileptic seizures in school-age children: educational project dedicated to school staff. Epilepsy Behav. 2020;105:106951. https://doi.org/10.1016/j.yebeh.2020.106951
- Friedman MJ, Sharieff GQ. Seizures in children. Pediatr Clin North Am. 2006;53:257-77. https://doi.org/10.1016/j.pcl.2005.09.010
- Fernandes PT, Noronha ALA, Araújo U, et al. Teachers perception about epilepsy. Arq Neuropsiquiatr. 2007;65(Suppl 1):28-34. https://doi.org/10.1590/s0004-282x2007001000005
- Al-Khateeb JM, Al-Khateeb AJ. Research on psychosocial aspects of epilepsy in Arab countries: a review of literature. Epilepsy Behav. 2014;31:256-62. https://doi.org/10.1016/j.yebeh.2013.09.033
- Chong L, Jamieson NJ, Gill D, et al. Children’s experiences of epilepsy: a systematic review of qualitative studies. Pediatrics. 2016;138:e20160658. https://doi.org/10.1542/peds.2016-0658
- Hsieh LP, Chiou HH. Comparison of epilepsy and asthma perception among preschool teachers in Taiwan. Epilepsia. 2001;42:647-50. https://doi.org/10.1046/j.1528-1157.2001.39200.x
- Alkhotani AM, Almalki WM, Alkhotani AM, Turkistani MA. Makkah female teachers’ knowledge of seizure first aid. Epilepsy Behav. 2019;98:10-3. https://doi.org/10.1016/j.yebeh.2019.05.047
- Papathanasopoulos PG, Tsibri ES, Gourzoulidou E, Konstantinou D. Near-deadly resuscitation during a grand mal seizure. Epilepsia. 2004;45:1164. https://doi.org/10.1111/j.0013-9580.2004.21604.x
- Beal MD, Kinnear J, Anderson CR, Martin TD, Wamboldt R, Hooper L. The effectiveness of medical simulation in teaching medical students critical care medicine: a systematic review and meta-analysis. Simul Healthc. 2017;12:104-16. https://doi.org/10.1097/SIH.0000000000000189
- Cook DA, Hamstra SJ, Brydges R, et al. Comparative effectiveness of instructional design features in simulation-based education: systematic review and meta-analysis. Med Teach. 2013;35:e867-98. https://doi.org/10.3109/0142159X.2012.714886
- İşler A, Başbakkal Z, Tosun AF, Tekgül H. Modüler eğitim modeli ile epileptik nöbeti olan çocuğa yaklaşım. Turkiye Klinikleri Journal of Neurology. 2011;6:46-8.
- Dean AG. OpenEpi: open source epidemiologic statistics for public health, version 2.3.1. 2010. Available at: http://www.openepi.com
- Adal O, Abebe A. First aid knowledge and practice toward students with epileptic seizure among governmental high school teachers in Addis Ababa, Ethiopia: cross-sectional study. Epilepsy Behav. 2022;134:108767. https://doi.org/10.1016/j.yebeh.2022.108767
- Singh G, Braga P, Carrizosa J, et al. An epilepsy curriculum for primary health care providers: a report from the Education Council of the International League Against Epilepsy. Epileptic Disord. 2022;24:983-93. https://doi.org/10.1684/epd.2022.1479
- George D. SPSS for windows step by step: a simple study guide and reference, 17.0 update, 10/e. India: Pearson Education; 2011.
- Beghi E. Social functions and socioeconomic vulnerability in epilepsy. Epilepsy Behav. 2019;100:106363. https://doi.org/10.1016/j.yebeh.2019.05.051
- Jones C, Atkinson P, Helen Cross J, Reilly C. Knowledge of and attitudes towards epilepsy among teachers: a systematic review. Epilepsy Behav. 2018;87:59-68. https://doi.org/10.1016/j.yebeh.2018.06.044
- Özlü ZK, Aras GU, Özlü İ, et al. Öğretmenlerin ilk yardım konusundaki bilgi düzeylerinin belirlenmesi. Anatolian Journal of Health Research 2022;3:139-43. https://doi.org/10.29228/anatoljhr.64990
- Yilmazel G. Teachers’ negative attitudes and limited health literacy levels as risks for low awareness of epilepsy in Turkey. J Prev Med Public Health. 2023;56:573-82. https://doi.org/10.3961/jpmph.23.330
- Örs M. Learning needs of primary schools teachers about first aid. Kastamonu Education Journal 2021;29:682-93. https://doi.org/10.24106/kefdergi.902282
- Soslu R, Elçi G, Özkan A. Beden eğitimi ve spor yüksekokulu öğrencı̇lerinin epilepsiye ilişkin bilgi düzeylerinin incelenmesi. CBÜ Beden Eğitimi ve Spor Bilimleri Dergisi. 2018;13:106-14.
- Üçer H, Sucaklı MH, Çelik M, Keten HS. Primary school teachers’ knowledge, attitudes and behaviors about childhood epilepsy. Cukurova Medical Journal. 2016;41:491-5. https://doi.org/10.17826/cukmedj.237491
- Orhan Sİ, Aydın A. Öğretmen adaylarının ilk yardım bilgi düzeyleri: Kastamonu üniversitesi örneği. Kastamonu Education Journal. 2020;28:1657-67. https://doi.org/10.24106/kefdergi.3798
- Alkhotani AM, Alkhotani AM. Effect of health education on female primary school teachers’ knowledge of seizure first aid: an interventional study. Epilepsy Behav. 2022;127:108523. https://doi.org/10.1016/j.yebeh.2021.108523
- Kampra M, Tzerakis NG, Losidis S, et al. Teachers’ knowledge about epilepsy in Greece: information sources and attitudes towards children with epilepsy during school time. Epilepsy Behav. 2016;60:218-24. https://doi.org/10.1016/j.yebeh.2016.04.004
- AlMuslim N, Aldawood M, Almulhim I, et al. Knowledge of epilepsy and seizure first aid among teachers in Eastern Province, Saudi Arabia. Cureus. 2023;15. https://doi.org/10.7759/cureus.33418
- Al-Hashemi E, Ashkanani A, Al-Qattan H, et al. Knowledge about epilepsy and attitudes toward students with epilepsy among middle and high school teachers in Kuwait. Int J Pediatr. 2016;2016:5138952. https://doi.org/10.1155/2016/5138952
- Elhassan MA, Alemairy AA, Amara ZM, Hamadelneel AA, Mohamed AH, Elaimeri AA. Epilepsy: knowledge, attitude, and practice among secondary school teachers in Khartoum State. Neurol Ther. 2017;6:225-35. https://doi.org/10.1007/s40120-017-0083-7
- Hirsch E, French J, Scheffer IE, et al. ILAE definition of the idiopathic generalized epilepsy syndromes: position statement by the ILAE task force on nosology and definitions. Epilepsia. 2022;63:1475-99. https://doi.org/10.1111/epi.17236
- Trinka E, Cock H, Hesdorffer D, et al. A definition and classification of status epilepticus-report of the ILAE task force on classification of status epilepticus. Epilepsia. 2015;56:1515-23. https://doi.org/10.1111/epi.13121
- Njamnshi AK, Angwafor SA, Baumann F, Angwafo FF, Jallon P, Muna WFT. Knowledge, attitudes, and practice of Cameroonian medical students and graduating physicians with respect to epilepsy. Epilepsia. 2009;50:1296-9. https://doi.org/10.1111/j.1528-1167.2009.02155.x
- Tavares TP, Kerr EN, Secco M, Bax K, Smith ML. Brief video enhances teacher trainees’ knowledge of epilepsy. Epilepsy Behav. 2021;118:107963. https://doi.org/10.1016/j.yebeh.2021.107963
- Farwana R, Sheriff A, Manzar H, Farwana M, Yusuf A, Sheriff I. Watch this space: a systematic review of the use of video-based media as a patient education tool in ophthalmology. Eye (Lond). 2020;34:1563-9. https://doi.org/10.1038/s41433-020-0798-z
- Abu Abed M, Himmel W, Vormfelde S, Koschack J. Video-assisted patient education to modify behavior: a systematic review. Patient Educ Couns. 2014;97:16-22. https://doi.org/10.1016/j.pec.2014.06.015
- Akgün M, Sekerci N, Demirdağ H, Doğan R. Okul öncesi öğretmenlerinin temel ilk yardım bilgi düzeylerinin belirlenmesi. Haliç Üniversitesi Sağlık Bilimleri Dergisi. 2023;6:30-8. https://doi.org/10.48124/husagbilder.1180096
Copyright and license
Copyright © 2026 The author(s). This is an open-access article published by Aydın Pediatric Society under the terms of the Creative Commons Attribution License (CC BY) which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.